 PDF
PDF  Views
Views  Share
Share


KRAS and NRAS Testing in Metastatic Colorectal Cancer in Central Iran (Tehran): A Review on Literature of the Middle East
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2018; 39(02): 210-214
DOI: DOI: 10.4103/ijmpo.ijmpo_133_17
Abstract
Context: The incidence of colorectal cancer (CRC) in the past three decades in Iran has made it as a major public health burden. Aims: The aim of this study is to report the prevalence of KRAS and NRAS mutations in Iran and the correlation between KRAS mutation status with clinicopathological factors and survival.Materials and Methods: In a cross-sectional study, 144 patients were entered into the study based on the criteria. Age, sex, tumor site, grade, metastasis location, familial history, KRAS/NRAS status, and survival were checked for all patients, and the patients were followed for 1 year. DNA was extracted with FFPE QIAGEN kit and then polymerase chain reaction for amplification of gene segments of KRAS and NRAS genes. Results: The mean age at diagnosis was 52.9 years (range: 27–72 years) that 39.6% patients had age <50 class="b" xss=removed>Conclusions: The metastatic CRC was more prevalent in men than women, and the mean age varied around 50–60 years. The results showed that the present study had the highest prevalence of KRAS mutation in the Middle East and Pakistan with the lowest prevalence in CRC patients.
Publication History
Article published online:
23 June 2021
© 2018. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Abstract
Context: The incidence of colorectal cancer (CRC) in the past three decades in Iran has made it as a major public health burden. Aims: The aim of this study is to report the prevalence of KRAS and NRAS mutations in Iran and the correlation between KRAS mutation status with clinicopathological factors and survival.Materials and Methods: In a cross-sectional study, 144 patients were entered into the study based on the criteria. Age, sex, tumor site, grade, metastasis location, familial history, KRAS/NRAS status, and survival were checked for all patients, and the patients were followed for 1 year. DNA was extracted with FFPE QIAGEN kit and then polymerase chain reaction for amplification of gene segments of KRAS and NRAS genes. Results: The mean age at diagnosis was 52.9 years (range: 27–72 years) that 39.6% patients had age <50 class="b" xss=removed>Conclusions: The metastatic CRC was more prevalent in men than women, and the mean age varied around 50–60 years. The results showed that the present study had the highest prevalence of KRAS mutation in the Middle East and Pakistan with the lowest prevalence in CRC patients.
Keywords
Colorectal cancer - Iran - KRAS - NRAS
Introduction
Colorectal cancer (CRC) is one of the most common cancers and is the second leading cause of cancer death in men and women in the United States and also is third common cancer in women and fifth in Iranian men.[1] The increasing incidence of CRC in the past three decades in Iran has made it as a major public health burden.[2] In CRC patients, metastases are the main cause of cancer-related mortality.[3] The most common sites of metastasis from colon cancer are the regional lymph nodes, the liver, the lung, and the peritoneum.[3],[4] Distant metastatic disease is present in approximately 25% of patients at initial diagnosis, and half of CRC patients will develop metastatic disease.[5] Most patients with metastatic CRC (mCRC) have an incurable disease.[3] The treatment of mCRC is one of the biggest successes in recent decades.[6] Targeted cancer therapy is becoming a powerful strategy for the treatment of patients selected on the basis of their molecular characteristics. This is particularly true for patients with mCRC.[2] RAS mutations are useful markers for predicting responses to anti-epidermal growth factor receptor monoclonal antibodies in mCRC.[2],[7] KRAS mutation varies between 20% and 50% in the most countries in the world,[8] but NRAS mutations are rare and occur in 3% and 5% of CRC.[9] The frequency of NRAS mutations and their relationship to clinical, pathologic, and molecular features remains uncertain.[9]
The aim of this study is another report from the prevalence of KRAS and NRAS mutations in Iran and the correlation between KRAS mutation status with clinicopathological factors and survival.
Materials and Methods
Patients
The cross-sectional study was done in CRC patients in Rasool Akram Hospital, Tehran, in 1 year (April 2015 to April 2016) that 144 patients were entered into the study based on inclusion criteria.
Inclusion criteria
Patients having mCRC and history of treatment with chemotherapy regimens were included in the study. Age, sex, tumor site, grade, metastasis location, familial history, KRAS/NRAS status, and survival were checked for all patients. The patients were followed up for 1 year. The overall survival was defined as the length of time from either the date of diagnosis or the start of treatment for cancer until death for any cause or the date of the last follow-up.
Extraction and amplification of KRAS/NRAS
Mutations and oncogenes of KRAS and NRAS of codons 12 and 13 were checked on fresh frozen and formalin-fixed paraffin-embedded (FFPE) tissues in Partolab Laboratory, Tehran, Iran. After 4–5 cutting with 2–5 μm thickness, DNA was extracted with FFPE QIAGEN kit, and then, polymerase chain reaction (P CR) for amplification of gene segments was done with an initial denaturation at 95°C for 11 min, denaturation at 95°C for 30 s, fusion at 55°C for 30 s, elongation at 72°C for 30 s, and end elongation at 72°C for 5 min. After electrophoresis of PCR products, a band in the situation of 120 bp was seen that is indicating amplification of gene segment during PCR. To ensure amplified fragment length to confirm the target gene, evaluation was performed by Gene Runner program, and the incision with enzyme was confirmed by MapViewer program. After that, using RFLP technic and suitable enzymes (Bgl1), the status of mutation and wild type was determined. The results again were checked with high-resolution melting analysis. KRAS and NRAS genes were analyzed and sequenced (pyrosequencing) by allele specific.
Statistical analysis
The analysis was done with IBM SPSS software version 22 (IBM Corp., Armonk, NY, USA) that t-test was used for the comparison of means between groups and Chi-square test for other variables. The overall survival was plotted and analyzed by Kaplan – Meier.
Results
The mean age ± standard deviation at diagnosis was 52.9 ± 12.7 years (range: 27–72 years) that 39.6% patients had age <50 href="https://www.thieme-connect.com/products/ejournals/html/10.4103/ijmpo.ijmpo_133_17#TB_1" xss=removed>Table 1]. Sigmoid (33.4%), ascending colon (31.2%), rectum (20.8%), descending colon (8.4%), and transverse colon (6.2%) were the highest tumor site in the patients. Grades I (well differentiated), II (moderate differentiated), and III (poorly differentiated) were 16.7%, 64.6%, and 18.7%, respectively. In all patients, liver metastasis (72.9%) had the highest prevalence, followed by nonregional lymph node and lung (each 10.4%) and other metastases (6.3%). Of 144 patients, 15 patients had a familial history of cancer, 72 (52.1%) had KRAS mutation, and 6 (4.2%) had NRAS mutation. In addition, during 1-year follow-up, 51 (35.4%) patients died for any cause.
|
Variables |
n (%) |
|---|---|
|
SD – Standard deviation; KRAS – Kirsten ras; NRAS – Neuroblastoma ras |
|
|
Age (years) |
|
|
Mean±SD |
52.9±12.7 |
|
Range |
27-72 |
|
<50> |
57 (39.6) |
|
Sex |
|
|
Male |
78 (54.2) |
|
Female |
66 (45.8) |
|
Tumor site |
|
|
Ascending colon |
45 (31.2) |
|
Transverse colon |
9 (6.2) |
|
Descending colon |
12 (8.4) |
|
Sigmoid |
48 (33.4) |
|
Rectum |
30 (20.8) |
|
Grade |
|
|
I |
24 (16.7) |
|
II |
93 (64.6) |
|
III |
27 (18.7) |
|
Metastasis location |
|
|
Liver |
105 (72.9) |
|
Nonregional lymph node |
15 (10.4) |
|
Lung |
15 (10.4) |
|
Other |
9 (6.3) |
|
Familial history |
|
|
Yes |
15 (10.4) |
|
No |
129 (89.6) |
|
KRAS status |
|
|
Mutation |
75 (52.1) |
|
Wild type |
69 (47.9) |
|
NRAS status |
|
|
Mutation |
6 (4.2) |
|
Wild type |
138 (95.8) |
|
One-year survival |
|
|
Alive |
93 (64.6) |
|
Deceased |
51 (35.4) |
|
Variables |
KRAS mutation (n=75) (%) |
KRAS wild type (n=69) (%) |
P |
|---|---|---|---|
|
SD – Standard deviation; KRAS – Kirsten ras |
|||
|
Age (years) |
|||
|
Mean±SD |
54.64±13.11 |
51.09±12.04 |
0.093 |
|
<50> |
18 (24)/57 (76) |
39 (56.5)/30 (43.5) <0> |
|
|
Sex |
0.645 |
||
|
Male |
42 (56) |
36 (52.1) |
|
|
Female |
33 (44) |
33 (47.9) |
|
|
Tumor site |
0.574 |
||
|
Ascending colon |
24 (32) |
21 (30.4) |
|
|
Transverse colon |
6 (8) |
3 (4.3) |
|
|
Descending colon |
6 (8) |
6 (8.7) |
|
|
Sigmoid |
21 (28) |
27 (39.2) |
|
|
Rectum |
18 (24) |
12 (17.4) |
|
|
Grade |
0.914 |
||
|
I |
12 (16) |
12 (17.4) |
|
|
II |
48 (64) |
45 (65.2) |
|
|
III |
15 (20) |
12 (17.4) |
|
|
Metastasis location |
0.436 |
||
|
Liver |
57 (76) |
48 (69.5) |
|
|
Nonregional |
6 (8) |
9 (13.1) |
|
|
lymph node Lung |
9 (12) |
6 (8.7) |
|
|
Other |
3 (4) |
6 (8.7) |
|
|
Familial history |
0.322 |
||
|
Yes |
6 (8) |
9 (13.1) |
|
|
No |
69(92) |
60 (86.9) |
|
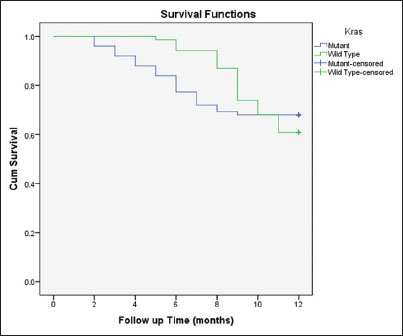
| Figure. 1The comparison of 1-year overall survival based on KRAS status
Discussion
This study showed that the prevalence of KRAS and NRAS mutations in mCRC patients in an Iranian population was 52.1% and 4.2%, respectively. Furthermore, KRAS mutation had significantly more prevalence in lower ages compared with KRAS wild type.
One study [10] in Western Iran on 83 mCRC patients (mean age: 57.7 years, range: 18–80 years, and 61.4% males) and another study on 33 mCRC patients [11] (mean age: 51.5 years, range: 22–76, and 79% males) in this area reported that the prevalence of KRAS mutation was 33.3% and 44.6%, respectively. Furthermore, there were no significant differences between patients with KRAS mutation and wild type in 5-(69% vs. 64%)[10] and 2-year (63% vs. 73%) overall survivals.[11] Two studies [10],[11] showed that the prevalence of clinicopathological factors in patients with KRAS mutation and wild type was similar. Two studies in Tehran (Central Iran)[1],[12] evaluated mCRC patients for KRAS status that the first study selected 1000 cases (57.3% males) with the prevalence of 33.6% for KRAS mutation, and the second study selected 182 CRC patients with the prevalence of 37.4% for KRAS mutation. Koochak et al.[13] indicate that KRAS mutations occurred at a statistically higher frequency in older patients (>50) than in younger patients (≤50) (P = 0.0001). It is also worth mentioning that KRAS mutation tended to occur at a more frequency in male cases than in female cases. KRAS mutations occur at a higher rate in pT3 than others (P = 0.0001). The studies in other areas of Iran reported 32% KRAS mutation in 100 cases (mean age: 59 years and 55% males) in Southern Iran,[14] 32.2% in 211 cases in Northern Iran,[13] and 28% in 50 cases (mean age: 60.8 years), and NRAS mutation was just in one case in codon 146 (2%) in Southern Iran.[15] The prevalence of NRAS mutation in Iranian CRC patients has been reported from 0%[6],[10],[11] to 4.2% (the present study). One review study [7] showed that the prevalence of KRAS mutation in Iran was between 30% and 50% (few studies reported 12.5%–37.4%) that this prevalence was similar to studies from other countries (20%–50%).
A total of 83 mCRC patients evaluated in Saudi Arabia [16] that 42.2% had KRAS mutation, and 51% and 23% of the tumors were from the left hemi-colon and rectum, respectively, 83% were moderately differentiated, and 86% were invasive adenocarcinoma. Another study on 300 CRC patients from Saudi Arabia [17] reported 42% KRAS mutation that mutations were associated with advanced stage of CRC and shorter recurrence-free survival and overall survival.
The studies reported in Turkey [18],[19],[20] checked 50, 172, and 53 mCRC patients. The prevalence of KRAS mutation was 30%, 44%, and 49.05%, respectively. KRAS mutation frequency was significantly higher in tumors located in the ascending colon,[18] and there was no difference in progression-free survival and overall survival between KRAS mutation and KRAS wild-type patients.
One hundred and fifty CRC patients (64% male) in Pakistan were assessed for KRAS status that 13% had the mutation, and this mutation seemed to be significantly associated with female patients.[21] One research in Egypt [22] analyzed KRAS status on 26 mCRC patients with immunohistochemistry. The results showed that 42.3% patients were KRAS mutation, and no significant correlation was found between clinicopathological parameters and KRAS staining results.[22] In Oman,[23] 79 CRC patients were checked that 48.1% had mutation and no relation was noticed with wild-type or mutant KRAS with recurrence-free survival and overall survival. In Iraq,[24] fifty CRC patients (mean age: 55.4 years and 54% males) enrolled that 48% had KRAS mutation, and there were no significant associations of age, gender, tumor location or histology, grading, staging, or lymphovascular invasion with KRAS mutation status.In the present study, there was no significant difference between clinicopathological factors with KRAS mutation status, except for age that KRAS mutation frequency was higher in age ≥50 years. Furthermore, there was no significant difference between KRAS mutation status for 1-year overall survival, but 6-month overall survival was significantly shorter in KRAS mutation compared with KRAS wild type.
Discussion
The mCRC was more prevalent in men than women, and the mean age varied around 50–60 years. The results showed that the present study had the highest prevalence of KRAS mutation in the Middle East and Pakistan with the lowest prevalence in CRC patients. The studies reported that survival of the patients was similar between KRAS mutation and wild type, but in the present study, 6-month survival had a significant difference. In the future, studies can be considered to the survivals of shorter than 1 year in mCRC patients. In addition to, in more studies, there was no significant difference between KRAS mutation status with clinicopathological factors but can be considered to the role of age, stage, and tumor location in the future studies.
Conflict of Interest
There are no conflicts of interest.
References
- hahriari-Ahmadi A, Fahimi A, Payandeh M, Sadeghi M. Prevalence of oxaliplatin-induced chronic neuropathy and influencing factors in patients with colorectal cancer in Iran. Asian Pac J Cancer Prev 2015; 16: 7603-6
- olatkhah R, Somi MH, Bonyadi MJ, Asvadi KermaniI, Farassati F, Dastgiri S. et al. Colorectal cancer in Iran: Molecular epidemiology and screening strategies. J Cancer Epidemiol 2015; 2015: 643020
- atandoust S, Price TJ, Karapetis CS. Colorectal cancer: Metastases to a single organ. World J Gastroenterol 2015; 21: 11767-76
- ayandeh M, Sadeghi M, Sadeghi E. The report of KRAS mutation and NRAS wild type in a patient with thyroid metastasis from colon cancer: A Rare case report. Iran J Pathol 2016; 11: 71-5
- an CutsemE, Oliveira J. ESMO Guidelines Working Group. et al. Advanced colorectal cancer: ESMO clinical recommendations for diagnosis, treatment and follow-up. Ann Oncol 2009; 20 Suppl 4: 61-3
- ajpai J, Susan D, Patil V, Nair R, Ghosh J, Badwe RA. et al. Taxane combination chemotherapy in breast cancer: Experience from a tertiary cancer centre in India. Indian J Med Paediatr Oncol 2017; 38: 18-21
- ayandeh M, Sadeghi M, Sadeghi E, Gholami F. Analysis of KRAS, BRAF and NRAS in patients with colorectal cancer: The first report of Western Iran. Am J Cancer Prev 2015; 3: 19-22
- eramizadeh b. Molecular biomarkers of colorectal cancer: A review of published articles from Iran. Ann Colorectal Res 2015; 3: e30100
- rahara N, Baba Y, Nosho K, Shima K, Yan L, Dias-Santagata D. et al. NRAS mutations are rare in colorectal cancer. Diagn Mol Pathol 2010; 19: 157-63
- Payandeh M, Shazad B, Sadeghi M, Shahbazi M. Correlation between RAS test results and prognosis of metastatic colorectal cancer patients: A Report from Western Iran. Asian Pac J Cancer Prev 2016; 17: 1729-32
- Amirifard N, Sadeghi E, Farshchian N, Haghparast A, Choubsaz M. Evaluation of KRAS gene mutations in metastatic colorectal cancer patients in Kermanshah province. Asian Pac J Cancer Prev 2016; 17: 3085-8
- Bishehsari F, Mahdavinia M, Malekzadeh R, Verginelli F, Catalano T, Sotoudeh M. et al. Patterns of K-ras mutation in colorectal carcinomas from Iran and Italy (a Gruppo Oncologico Dell'italia Meridionale study): Influence of microsatellite instability status and country of origin. Ann Oncol 2006; 17 Suppl 7: vii91-6
- Koochak A, Rakhshani N, Karbalaie NiyaMH, Tameshkel FS, Sohrabi MR, Babaee MR. et al. Mutation analysis of KRAS and BRAF genes in metastatic colorectal cancer: A First large scale study from Iran. Asian Pac J Cancer Prev 2016; 17: 603-8
- Omidifar NMd, Geramizadeh GMd, Mirzai MMs. K-ras mutation in colorectal cancer, A report from Southern Iran. Iran J Med Sci 2015; 40: 454-60
- Mohsen A, Ahmadreza S, Fatemeh H, Fatemeh H, Fariba ER. et al. Frequency of K-RAS and N-RAS gene mutations in colorectal cancers in Southeastern Iran. Asian Pac J Cancer Prev 2016; 17: 4511-5
- Bader T, Ismail A. Higher prevalence of KRAS mutations in colorectal cancer in Saudi Arabia: Propensity for lung metastasis. Alexandria J Med 2014; 50: 203-9
- Zekri J, Al-Shehri A, Mahrous M, Al-Rehaily S, Darwish T, Bassi S. et al. Mutations in codons 12 and 13 of K-ras exon 2 in colorectal tumors of Saudi Arabian patients: Frequency, clincopathological associations, and clinical outcomes. Genet Mol Res 2017; 16: 1-11
- Gorukmez O, Yakut T, Gorukmez O, Sag SO, Karkucak M, Kanat O. et al. Distribution of KRAS and BRAF mutations in metastatic colorectal cancers in Turkish patients. Asian Pac J Cancer Prev 2016; 17: 1175-9
- Selcukbiricik F, Erdamar S, Ozkurt CU, Molinas MandelN, Demirelli F, Ozguroglu M. et al. The role of K-RAS and B-RAF mutations as biomarkers in metastatic colorectal cancer. J BUON 2013; 18: 116-23
- Ozen F, Ozdemir S, Zemheri E, Hacimuto G, Silan F, Ozdemir O. et al. The proto-oncogene KRAS and BRAF profiles and some clinical characteristics in colorectal cancer in the Turkish population. Genet Test Mol Biomarkers 2013; 17: 135-9
- Murtaza BN, Bibi A, Rashid MU, Khan YI, Chaudri MS, Shakoori AR. et al. Spectrum of K ras mutations in Pakistani colorectal cancer patients. Braz J Med Biol Res 2014; 47: 35-41
- Elsabah MT, Adel I. Immunohistochemical assay for detection of K-ras protein expression in metastatic colorectal cancer. J Egypt Natl Canc Inst 2013; 25: 51-6
- Kumar S, Burney IA, Zahid KF, DSouza PC, Belushi MA, Mufti TD. et al. Colorectal cancer patient characteristics, treatment and survival in Oman – A single center study. Asian Pac J Cancer Prev 2015; 16: 4853-8
- Al-Allawi NA, Ismaeel AT, Ahmed NY, Merza NS. The frequency and spectrum of K-ras mutations among Iraqi patients with sporadic colorectal carcinoma. Indian J Cancer 2012; 49: 163-8
Address for correspondence
Publication History
Article published online:
23 June 2021
© 2018. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2,
Noida-201301 UP, India
| Figure. 1The comparison of 1-year overall survival based on KRAS status
References
- hahriari-Ahmadi A, Fahimi A, Payandeh M, Sadeghi M. Prevalence of oxaliplatin-induced chronic neuropathy and influencing factors in patients with colorectal cancer in Iran. Asian Pac J Cancer Prev 2015; 16: 7603-6
- olatkhah R, Somi MH, Bonyadi MJ, Asvadi KermaniI, Farassati F, Dastgiri S. et al. Colorectal cancer in Iran: Molecular epidemiology and screening strategies. J Cancer Epidemiol 2015; 2015: 643020
- atandoust S, Price TJ, Karapetis CS. Colorectal cancer: Metastases to a single organ. World J Gastroenterol 2015; 21: 11767-76
- ayandeh M, Sadeghi M, Sadeghi E. The report of KRAS mutation and NRAS wild type in a patient with thyroid metastasis from colon cancer: A Rare case report. Iran J Pathol 2016; 11: 71-5
- an CutsemE, Oliveira J. ESMO Guidelines Working Group. et al. Advanced colorectal cancer: ESMO clinical recommendations for diagnosis, treatment and follow-up. Ann Oncol 2009; 20 Suppl 4: 61-3
- ajpai J, Susan D, Patil V, Nair R, Ghosh J, Badwe RA. et al. Taxane combination chemotherapy in breast cancer: Experience from a tertiary cancer centre in India. Indian J Med Paediatr Oncol 2017; 38: 18-21
- ayandeh M, Sadeghi M, Sadeghi E, Gholami F. Analysis of KRAS, BRAF and NRAS in patients with colorectal cancer: The first report of Western Iran. Am J Cancer Prev 2015; 3: 19-22
- eramizadeh b. Molecular biomarkers of colorectal cancer: A review of published articles from Iran. Ann Colorectal Res 2015; 3: e30100
- rahara N, Baba Y, Nosho K, Shima K, Yan L, Dias-Santagata D. et al. NRAS mutations are rare in colorectal cancer. Diagn Mol Pathol 2010; 19: 157-63
- Payandeh M, Shazad B, Sadeghi M, Shahbazi M. Correlation between RAS test results and prognosis of metastatic colorectal cancer patients: A Report from Western Iran. Asian Pac J Cancer Prev 2016; 17: 1729-32
- Amirifard N, Sadeghi E, Farshchian N, Haghparast A, Choubsaz M. Evaluation of KRAS gene mutations in metastatic colorectal cancer patients in Kermanshah province. Asian Pac J Cancer Prev 2016; 17: 3085-8
- Bishehsari F, Mahdavinia M, Malekzadeh R, Verginelli F, Catalano T, Sotoudeh M. et al. Patterns of K-ras mutation in colorectal carcinomas from Iran and Italy (a Gruppo Oncologico Dell'italia Meridionale study): Influence of microsatellite instability status and country of origin. Ann Oncol 2006; 17 Suppl 7: vii91-6
- Koochak A, Rakhshani N, Karbalaie NiyaMH, Tameshkel FS, Sohrabi MR, Babaee MR. et al. Mutation analysis of KRAS and BRAF genes in metastatic colorectal cancer: A First large scale study from Iran. Asian Pac J Cancer Prev 2016; 17: 603-8
- Omidifar NMd, Geramizadeh GMd, Mirzai MMs. K-ras mutation in colorectal cancer, A report from Southern Iran. Iran J Med Sci 2015; 40: 454-60
- Mohsen A, Ahmadreza S, Fatemeh H, Fatemeh H, Fariba ER. et al. Frequency of K-RAS and N-RAS gene mutations in colorectal cancers in Southeastern Iran. Asian Pac J Cancer Prev 2016; 17: 4511-5
- Bader T, Ismail A. Higher prevalence of KRAS mutations in colorectal cancer in Saudi Arabia: Propensity for lung metastasis. Alexandria J Med 2014; 50: 203-9
- Zekri J, Al-Shehri A, Mahrous M, Al-Rehaily S, Darwish T, Bassi S. et al. Mutations in codons 12 and 13 of K-ras exon 2 in colorectal tumors of Saudi Arabian patients: Frequency, clincopathological associations, and clinical outcomes. Genet Mol Res 2017; 16: 1-11
- Gorukmez O, Yakut T, Gorukmez O, Sag SO, Karkucak M, Kanat O. et al. Distribution of KRAS and BRAF mutations in metastatic colorectal cancers in Turkish patients. Asian Pac J Cancer Prev 2016; 17: 1175-9
- Selcukbiricik F, Erdamar S, Ozkurt CU, Molinas MandelN, Demirelli F, Ozguroglu M. et al. The role of K-RAS and B-RAF mutations as biomarkers in metastatic colorectal cancer. J BUON 2013; 18: 116-23
- Ozen F, Ozdemir S, Zemheri E, Hacimuto G, Silan F, Ozdemir O. et al. The proto-oncogene KRAS and BRAF profiles and some clinical characteristics in colorectal cancer in the Turkish population. Genet Test Mol Biomarkers 2013; 17: 135-9
- Murtaza BN, Bibi A, Rashid MU, Khan YI, Chaudri MS, Shakoori AR. et al. Spectrum of K ras mutations in Pakistani colorectal cancer patients. Braz J Med Biol Res 2014; 47: 35-41
- Elsabah MT, Adel I. Immunohistochemical assay for detection of K-ras protein expression in metastatic colorectal cancer. J Egypt Natl Canc Inst 2013; 25: 51-6
- Kumar S, Burney IA, Zahid KF, DSouza PC, Belushi MA, Mufti TD. et al. Colorectal cancer patient characteristics, treatment and survival in Oman – A single center study. Asian Pac J Cancer Prev 2015; 16: 4853-8
- Al-Allawi NA, Ismaeel AT, Ahmed NY, Merza NS. The frequency and spectrum of K-ras mutations among Iraqi patients with sporadic colorectal carcinoma. Indian J Cancer 2012; 49: 163-8