 PDF
PDF  Views
Views  Share
Share


Metaplastic carcinoma of the breast with rhabdo-myosarcomatous element
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2014; 35(01): 117-118
DOI: DOI: 10.4103/0971-5851.133738
|
Publication History
Article published online:
19 July 2021
© 2014. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Sir,
Metaplastic carcinoma of the breast is malignant breast neoplasm composed of a mixture of both epithelial and mesenchymal elements. It accounts for 0.2% of all breast carcinomas.[1] We report this entity in a 55-year-old lady who presented with a huge lump in her right breast since one year. On local examination, a 12 x 10 cm hard lump was seen involving almost the entire right breast with an ulceroproliferative nodule on the skin surface. Multiple enlarged mobile lymph nodes were found in the right axilla. Clinical diagnosis of carcinoma was made and modified radical mastectomy with axillary clearance was done.
The mastectomy specimen contained a 12×10×9 cm grey white fleshy mass with necrotic areas. The mass extended up to the skin surface in the upper outer quadrant with ulceration [Figure [Figure1a1a and andb].b]. The mass extended close to the posterior resection margin. The nipple and areola appeared unremarkable. Dissection of the axillary tail revealed nine lymph nodes.
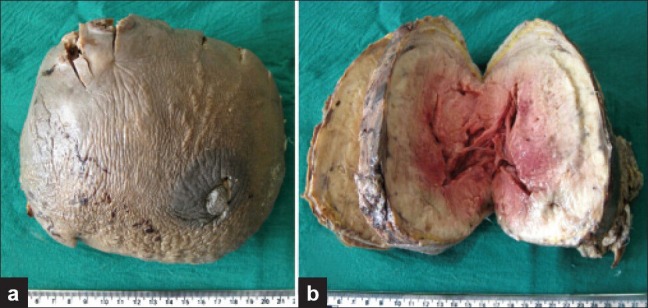
| Figure 1:(a) Gross photograph of the breast specimen showing ulceration of the skin surface; (b) Cut section of the tumor showing grey white fish-flesh like appearance with areas of necrosis and hemorrhage
Microscopy revealed a pleomorphic malignant tumor comprised of both epithelial and mesenchymal elements. The cells were arranged in sheets, nests, and cords. Binucleated and multinucleated tumor cells were evident. Few tumor cells had abundant granular eosinophilic cytoplasm. Many abnormal mitotic figures were also noted [Figure 2]. The tumor cells were infiltrating up to the overlying skin Three of the nine axillary lymph nodes showed tumor deposits. Immunohistochemistry showed that the tumor cells were reactive for vimentin [Figure 3], desmin, and cytokeratin; and were negative for estrogen receptor (ER), progesterone receptor (PR), and Her-2/neu. Based on the above features, the tumor was diagnosed as metaplastic carcinoma with rhabdomyosarcomatous element.
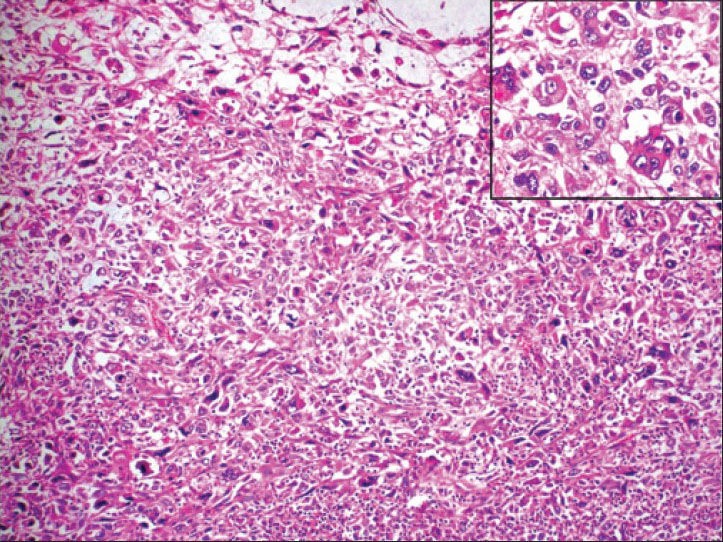
| Figure 2:Photomicrograph showing pleomorphic malignant tumor comprised of both epithelial and mesenchymal elements (H and E, ×100). The inset shows tumor cells with abundant granular eosinophilic cytoplasm (H and E, 400)
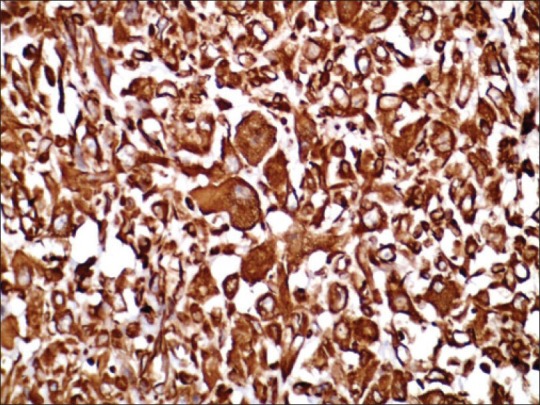
| Figure 3:Axial fused PET/CT images show FDG avid metastatic lesions in brain (a – arrow), left iliac marrow (b – arrow), D12Tumor cells showing strong cytoplasmic positivity for vimentin (×400)
Metaplastic carcinoma of the breast is a rare breast tumor. The median age of presentation in a series of 19 patients was 48 years and 50.5 years in another series of 14 cases.[2] In the present case, the patient was aged 55 years. Most of these tumors present as large, firm, nodular masses, often measuring up to 5 cm in diameter. Fixation to skin or deep fascia is common.[1] The tumor shows varying proportions of carcinomatous and pseudosarcomatous elements. The sarcoma-like component may resemble malignant fibrous histiocytoma, chondrosarcoma, osteosarcoma, rhabdomyosarcoma, or a combination of these.[3] Most metaplastic carcinomas are negative for ER, PR, and HER-2/neu,[3] which was also seen in the present case. These tumors are managed by radical mastectomy, followed by radiation and chemotherapy. The present case is doing well in postmastectomy period and is receiving chemotherapy at present. Metaplastic carcinoma is an aggressive form of breast cancer associated with poor outcome, high incidence of local recurrence, and pulmonary metastasis. The tumor size has an important impact on outcome. In a series of 19 females studied, the median tumor size was 9 cm, with the three-year event-free survival of 15%.[2]
Although metaplastic carcinoma of the breast can be difficult to establish both on clinical and histopathological basis, it should be diagnosed and excised at the earliest as it has an aggressive course and poor outcome.
Metaplastic carcinoma of the breast is a rare breast tumor. The median age of presentation in a series of 19 patients was 48 years and 50.5 years in another series of 14 cases.[2] In the present case, the patient was aged 55 years. Most of these tumors present as large, firm, nodular masses, often measuring up to 5 cm in diameter. Fixation to skin or deep fascia is common.[1] The tumor shows varying proportions of carcinomatous and pseudosarcomatous elements. The sarcoma-like component may resemble malignant fibrous histiocytoma, chondrosarcoma, osteosarcoma, rhabdomyosarcoma, or a combination of these.[3] Most metaplastic carcinomas are negative for ER, PR, and HER-2/neu,[3] which was also seen in the present case. These tumors are managed by radical mastectomy, followed by radiation and chemotherapy. The present case is doing well in postmastectomy period and is receiving chemotherapy at present. Metaplastic carcinoma is an aggressive form of breast cancer associated with poor outcome, high incidence of local recurrence, and pulmonary metastasis. The tumor size has an important impact on outcome. In a series of 19 females studied, the median tumor size was 9 cm, with the three-year event-free survival of 15%.[2]
Although metaplastic carcinoma of the breast can be difficult to establish both on clinical and histopathological basis, it should be diagnosed and excised at the earliest as it has an aggressive course and poor outcome.
References
- Hemalatha AL, Rao S, Nataraju G, Kumar BD, Shashidhar HB. Metaplastic carcinoma of the breast-A rare neoplasm with transitional cell differentiation: An exceptional feature. Indian J Pathol Microbiol 2010;53:356-8.
- Al Sayed AD, El Weshi AN, Tulbah AM, Rahal MM, Ezzat AA. Metaplastic carcinoma of the breast clinical presentation, treatment, results and prognostic factors. Acta Oncol 2006;45:188-95.
- Juan R, editor. Breast. In: Rosai, Ackerman′s. Surgical Pathology. 9th ed. New Delhi (India): Thompson Press; 2004. p. 1763-876.
| Figure 1:(a) Gross photograph of the breast specimen showing ulceration of the skin surface; (b) Cut section of the tumor showing grey white fish-flesh like appearance with areas of necrosis and hemorrhage
| Figure 2:Photomicrograph showing pleomorphic malignant tumor comprised of both epithelial and mesenchymal elements (H and E, ×100). The inset shows tumor cells with abundant granular eosinophilic cytoplasm (H and E, 400)
| Figure 3:Axial fused PET/CT images show FDG avid metastatic lesions in brain (a – arrow), left iliac marrow (b – arrow), D12Tumor cells showing strong cytoplasmic positivity for vimentin (×400)
References
- Hemalatha AL, Rao S, Nataraju G, Kumar BD, Shashidhar HB. Metaplastic carcinoma of the breast-A rare neoplasm with transitional cell differentiation: An exceptional feature. Indian J Pathol Microbiol 2010;53:356-8.
- Al Sayed AD, El Weshi AN, Tulbah AM, Rahal MM, Ezzat AA. Metaplastic carcinoma of the breast clinical presentation, treatment, results and prognostic factors. Acta Oncol 2006;45:188-95.
- Juan R, editor. Breast. In: Rosai, Ackerman′s. Surgical Pathology. 9th ed. New Delhi (India): Thompson Press; 2004. p. 1763-876.