 PDF
PDF  Views
Views  Share
Share


A case of primary ovarian lymphoma with autoimmune hemolytic anemia achieving complete response with Rituximab-based combination chemotherapy
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2011; 32(04): 207-210
DOI: DOI: 10.4103/0971-5851.95142
Abstract
Ovarian involvement as primary or secondary lymphomatous process is extremely uncommon. In most cases, the diagnosis is usually not suspected initially and is confirmed only after detailed histopathological evaluation. We report a patient with primary ovarian diffuse large B-cell lymphoma (DLBCL) and associated auto-immune hemolytic anemia (AIHA) who achieved complete remission after treatment with Rituximab-cyclophosphamide-doxorubicin-vincristine and prednisolone (R-CHOP) chemotherapy. This patient was a 50 year old female, who presented with fever, abdominal pain, vomiting, weight loss and anemia. Computed tomography scan of the abdomen and pelvis revealed a large left ovarian mass with bilateral hydronephrosis. We performed exploratory laparotomy and partial resection of the mass was done due to the adhesions. Histopathology confirmed the diagnosis of DLBCL. After six R-CHOP chemotherapy cycles, patient achieved complete response with correction of anemia. To our knowledge, this may be the first case report till date of primary ovarian DLBCL with AIHA treated with R-CHOP chemotherapy who achieved complete remission in terms of primary disease as well as hemolytic anemia.
Publication History
Article published online:
06 August 2021
© 2011. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Abstract
Ovarian involvement as primary or secondary lymphomatous process is extremely uncommon. In most cases, the diagnosis is usually not suspected initially and is confirmed only after detailed histopathological evaluation. We report a patient with primary ovarian diffuse large B-cell lymphoma (DLBCL) and associated auto-immune hemolytic anemia (AIHA) who achieved complete remission after treatment with Rituximab-cyclophosphamide-doxorubicin-vincristine and prednisolone (R-CHOP) chemotherapy. This patient was a 50 year old female, who presented with fever, abdominal pain, vomiting, weight loss and anemia. Computed tomography scan of the abdomen and pelvis revealed a large left ovarian mass with bilateral hydronephrosis. We performed exploratory laparotomy and partial resection of the mass was done due to the adhesions. Histopathology confirmed the diagnosis of DLBCL. After six R-CHOP chemotherapy cycles, patient achieved complete response with correction of anemia. To our knowledge, this may be the first case report till date of primary ovarian DLBCL with AIHA treated with R-CHOP chemotherapy who achieved complete remission in terms of primary disease as well as hemolytic anemia.
INTRODUCTION
Ovarian involvement by non-Hodgkin's lymphoma (NHL) is rare occurrence.[1] Most of the literature available is in the form of case reports and a few case series.[2–4] Disseminated lymphomatous process can involve the ovaries as secondary involvement in about 7%-cases.[5] Primary ovarian lymphoma constitutes 0.5% of all NHL and 1.5% of all ovarian malignancies.[1]
Auto immune hemolytic anemia, AIHA associated with hematolymphoid malignancies although rare, is a typical complication. Almost all types of lymphomas are associated with AIHA.[6] Occurrence of AIHA with extranodal lymphoma is exceedingly rare.
Most of the cases and series of ovarian lymphoma have patients treated with cyclophosphamide, doxorubicin, vincristine and prednisolone CHOP or CHOP-like combination chemotherapies with or without surgery.[7–9]
Here, we describe a patient with primary ovarian diffuse large B cell lymphoma, DLBCL and AIHA who achieved complete remission after immunochemotherapy with Rituximab, a monoclonal antibody targeting CD-20 and CHOP chemotherapy (R-CHOP).
CASE REPORT
A 50-year-old female patient with past history of diabetes mellitus was admitted with a four-month history of fever, easy fatigability, significant weight loss (8 kg) and recent onset of abdominal pain. A physical examination revealed anemia and mild jaundice and per abdominal examination revealed a tender mass in the left iliac fossa reaching up to the umbilicus. Bimanual pelvic examination revealed a large smooth pelvic mass (size of 16 weeks’ gravid uterus). There was no recent history of blood transfusion.
Hemogram confirmed anemia (Hb 7.4 g/dL) with normal red blood cell (RBC) indices and erythrocyte sedimentation rate ESR of 110 mm at the end of the first hour. Iron studies, vitamin B12 and folic acid levels were normal. Peripheral smear examination showed many agglutinated RBCs with polychromasia and occasional nucleated RBC [Figure 1]. Reticulocyte count was 4% and direct Coomb's test was positive. Her other laboratory parameters showed raised total bilirubin with predominantly indirect hyperbilirubinemia (total bilirubin 2.5 mg/dL, indirect bilirubin 2 mg/dL), raised cancer antigen-125 (CA-125) level of 60 U/ml (normal less than 35 U/L), and high lactate dehydrogenase LDH levels of 756 U/L (normal up to 180 U/L). Renal parameters were normal.
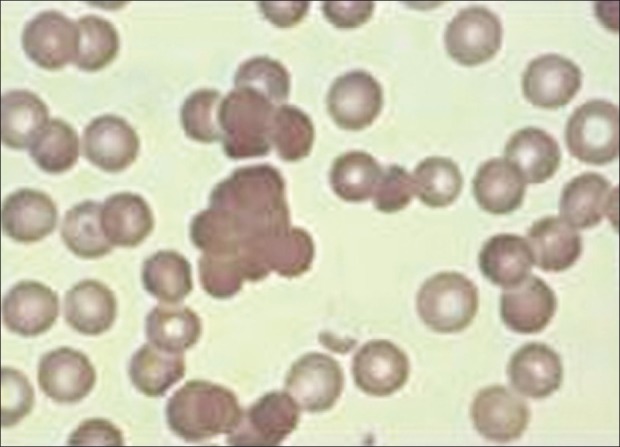
| Figure 1:Peripheral smear examination showing clumped RBCs suggestive of auto agglutination
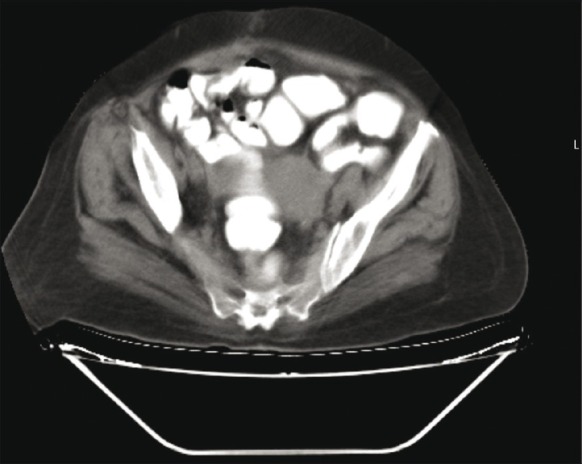
Computed tomography (CT) scan of the abdomen and pelvis with contrast studies confirmed the presence of a large, midline, lobulated, enhancing mass lesion of size 14×10 cm with central hypodense areas seen arising from the pelvis. The uterus and the ovaries could not be visualized separately. There was loss of fat planes between the mass and the rectum. There was bilateral hydronephrosis. Paraaortic lymph nodes were enlarged [Figure 2].
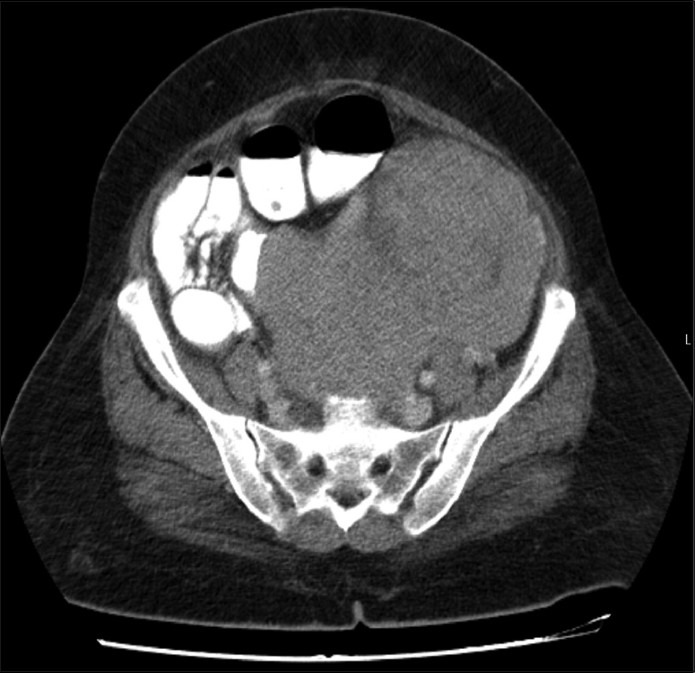
| Figure 2:Abdominopelvic CT scan showing large enhancing ovarian mass
Due to acute worsening of abdominal pain, patient was subjected to exploratory laparotomy through a midline incision. Subtotal resection of the mass was done as tumor was fixed to the adjacent structures. Patient also underwent bilateral ureteric stenting intraoperatively.
On gross examination, the single lobulated mass measured 11 × 8 × 8 cm with attached fallopian tube. Cut section was grey-white with areas of focal necrosis. The histopathological and immunohistochemistry studies confirmed the diagnosis of DLBCL of the ovary. Most of the neoplastic cells were leucocyte common antigen (LCA)-positive and showed diffuse strong membrane positivity for CD-20 antibody. Ki-67 labeling index was 50-55% [Figures [Figures33–5].
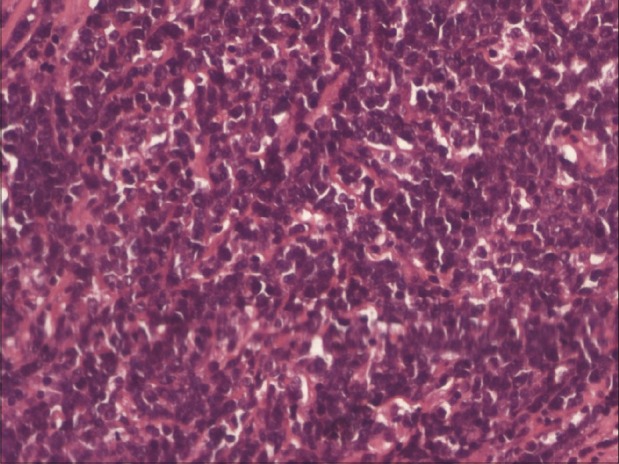
| Figure 3:Hematoxylin and eosin-stained section at ×20 magnification (low power) shows a lesion comprised of monotonous population of large cells diffusely infiltrating the stroma. No normal ovarian stroma could be identified
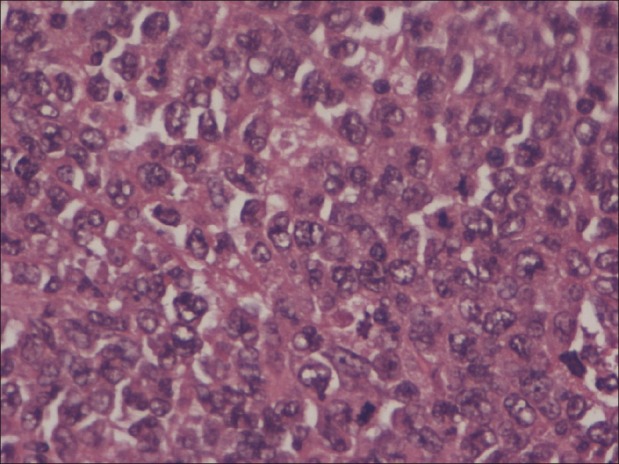
| Figure 4:Hematoxylin and eosin-stained section at ×40 magnification (high power) shows the cellular morphology. The cells have round to oval hyperchromatic nuclei with prominent nucleoli and scant cytoplasm. Mitotic activity is brisk
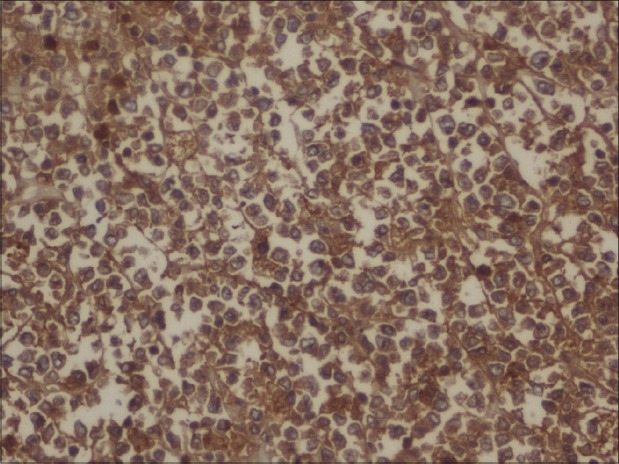
| Figure 5:Immunohistochemistry: CD 20-strong diffuse membrane positivity in round cells
Bone marrow biopsy was negative for lymphomatous involvement with erythroid hyperplasia. CT thorax was normal. This patient was staged as IIE according to the Ann Arbor staging system. Patient was treated with six cycles of R-CHOP chemotherapy, consisting of Rituximab (375 mg/m2 i.v.), cyclophosphamide (750 mg/m2 i.v.), doxorubicin (50 mg/m2 i.v.), vincristine (1.4 mg/2 i.v.) and presdnisolone (100 mg p.o on Days 1-5), every three weeks. Patient's hemoglobin increased to 10 g/dl post first cycle of R-CHOP chemotherapy with levels maintained above 10 g/dl throughout the treatment course. Peripheral smear examination was normal with no evidence of autoagglutination or hemolysis.
After completion of six R-CHOP cycles, patient achieved complete remission with normal imaging [Figure 6]. Patient received involved field radiotherapy post chemotherapy in view of bulky disease. Patient is disease-free at the end of six months from the initial surgery. There is no evidence of hemolysis at present.
| Figure 6:CT scan post six cycles of R-CHOP showing complete resolution of the disease
DISCUSSION
Ovarian lymphoma is indeed a rare disease. The very fact that ovaries are devoid of any lymphoid tissue raises doubts about the existence of this entity. Skodras et al., in their study of 37 oophorectomy specimens confirmed the presence of scattered lymphocytes and small lymphoid aggregates on immunohistochemistry.[9]
Ovarian involvement by a lymphomatous process can be primary or secondary of which the later can be disseminated lymphomas or occult extraovarian disease.[10] It is important to differentiate these two entities because outcomes are worse with the secondary lymphoma than primary ovarian lymphoma.[2]
Again, immune cytopenias are rare but known associations with hematolymphoid malignancies. A study by Moreno et al., confirmed a 7% incidence of immune cytopenias with 5% AIHA in chronic lymphocytic leukemia (CLL) patients.[11] This occurrence of AIHA with various lymphomas is also known but extremely rare with DLBCL.[6,12]
Till the approval of Rituximab in the treatment of B-cell lymphoma, CHOP chemotherapy was considered the standard of care.[13] With the current evidence, R-CHOP is considered as the new standard of care for any stage DLBCL. Still, there is paucity of evidence about the use of Rituximab in the treatment of B extranodal lymphoma including ovarian B-cell lymphoma. The literature of primary extranodal NHL treated with Rituximab-based chemoimmunotherapy comprises mainly case reports and small case series.[14–16]
In a case report, Komoto D described a patient of primary ovarian lymphoma achieving complete remission after three cycles of R-CHOP regimen.[17] Rajnics et al., treated three cases of primary genital non-ovarian lymphomas (two uterine and one prostatic lymphoma) with R-CHOP regimen with favorable outcome in young patients.[16] Signorelli et al., in their retrospective analysis had a patient with vaginal DLBCL treated with eight cycles of R-CHOP showing complete long-term remission.[18] In another study, there was no significant difference in treatment outcomes in primary ovarian lymphoma treated with CHOP or R-CHOP chemotherapy regimens.[19]
Interestingly, steroids are the first line of therapy for AIHA. Even in refractory cases of AIHA, Rituximab alone or in combination with steroids and cyclophosphamide has been used with favorable outcomes.[20–22]
In this case, R-CHOP chemotherapy, which is a standard treatment for DLBCL not only helped in achieving complete response for lymphoma but also to achieve AIHA remission.
In conclusion, this may be the first case report of primary ovarian diffuse large B-cell lymphoma with autoimmune hemolytic anemia achieving complete remission with R-CHOP chemotherapy.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- Dimopoulos MA, Daliani D, Pugh W, Gershenson D, Cabanillas F, Sarris AH. Primary ovarian non-Hodgkin′s lymphoma: Outcome after treatment with combination chemotherapy. Gynecol Oncol 1997;64:446-50.
- Osborne BM, Robboy SJ. Lymphomas or leukemia presenting as ovarian tumors. An analysis of 42 cases. Cancer 1983;52:1933-43.
- Lagoo AS, Robboy SJ. Lymphoma of the female genital tract: Current status. Int J Gynecol Pathol 2006;25:1-21.
- Kosari F, Daneshbod Y, Parwaresch R, Krams M, Wacker HH. Lymphomas of the female genital tract: A study of 186 cases and review of the literature. Am J Surg Pathol 2005;29:1512-20.
- Woodruff JD, NoliCastillord, Novak ER. Lymphoma of the ovary. A study of 35 cases from the Ovarian Tumor Registry of the American Gynecological Society. Am J Obstet Gynecol 1963;85:912-8.
- Hauswirth AW, Skrabs C, Schützinger C, Gaiger A, Lechner K, Jäger U. Autoimmune hemolytic anemias, Evans′ syndromes, and pure red cell aplasia in non-Hodgkin lymphomas. Leuk Lymphoma 2007;48:1139-49.
- Ambulkar I, Nair R. Primary ovarian lymphoma: Report of cases and review of literature. Leuk Lymphoma 2003;44:825-7.
- Monterroso V, Jaffe ES, Merino MJ, Medeiros LJ. Malignant lymphomas involving the ovary: A clinicopathologic analysis of 39 cases. Am J Surg Pathol 1993;17:154-70.
- Skodras G, Fields V, Kragel PJ. Ovarian lymphomas and serous carcinoma of low malignant potential arising in the same ovary: A case report with literature review of primary ovarian lymphoma. Arch Pathol Lab Med 1994;118:647-50.
- ;Ferry JA, Young RH. Malignant lymphomas, pseuso lymphomas and hematopoeitic disorders of the female genital tract. Pathol Ann 1991;26:227-63.
- ;Moreno C, Hodgson K, Ferrer G, Elena M, Filella X, Pereira A, et al. Autoimmune cytopenia in chronic lymphocytic leukemia: Prevalence, clinical associations, and prognostic significance. Blood 2010;116:4771-6.
- Eve HE, Rule SA. Autoimmune haemolyticanaemia associated with mantle cell lymphoma. Int J Hematol 2010;91:322-5.
- McKelvey EM, Gottlieb JA, Wilson HE, Haut A, Talley RW, Stephens R, et al. Hydroxyldaunomycin (Adriamycin) combination chemotherapy in malignant lymphoma. Cancer 1976;38:1484-93.
- Kim KM, Yoon DH, Lee SG, Lim SN, Sug LJ, Huh J, et al. A case of primary adrenal diffuse large B-cell lymphoma achieving complete remission with Rituximab -CHOP chemotherapy. J Korean Med Sci2009;24:525-8.
- Ferreri AJ, Dognini GP, Bairey O, Szomor A, Montalbán C, Horvath B, et al. The addition of rituximab to anthracycline-based chemotherapy significantly improves outcome in ′Western′ patients with intravascular large B-cell lymphoma. Br J Haematol 2008;143:253-7.
- Rajnics P, Demeter J, Csomor J, Krenács L, Pajor L, Kollár B, et al. Rare primary extranodal lymphomas: Diffuse large B-cell lymphomas of the genital tract. Ann Hematol 2009;88:1223-8.
- Komoto D, Nishiyama Y, Yamamoto Y, Monden T, Sasakawa Y, Toyama Y, et al. A case of non-Hodgkin′s lymphoma of the ovary: Usefulness of 18F-FDG PET for staging and assessment of the therapeutic response. Ann Nucl Med 2006;20:157-60.
- Signorelli M, Maneo A, Cammarota S, Isimbaldi G, Garcia Parra R, Perego P, et al. Conservative management in primary genital lymphomas: The role of chemotherapy. Gynecol Oncol 2007;104:416-21.
- Yun J, Kim SJ, Won JH, Choi CW, Eom HS, Kim JS, et al. Clinical features and prognostic relevance of ovarian involvement in non-Hodgkin′s lymphoma: A consortium for improving survival of lymphoma (CISL) report. Leuk Res 2010;34:1175-9.
- Peñalver FJ, Alvarez-Larrán A, Díez-Martin JL, Gallur L, Jarque I, Caballero D, et al. Rituximab is an effective and safe therapeutic alternative in adults with refractory and severe autoimmune hemolytic anemia. Ann Hematol 2010;89:1073-80.
- Kaufman M, Limaye SA, Driscoll N, Johnson C, Caramanica A, Lebowicz Y, et al. A combination of rituximab, cyclophosphamide and dexamethasone effectively treats immune cytopenias of chronic lymphocytic leukemia. Leuk Lymphoma 2009;50:892-9.
- Gupta V, Shukla J, Bhatia BD. Autoimmune hemolytic anemia. Indian J Pediatr 2008;75:451-4.
| Figure 1:Peripheral smear examination showing clumped RBCs suggestive of auto agglutination
| Figure 2:Abdominopelvic CT scan showing large enhancing ovarian mass
| Figure 3:Hematoxylin and eosin-stained section at ×20 magnification (low power) shows a lesion comprised of monotonous population of large cells diffusely infiltrating the stroma. No normal ovarian stroma could be identified
| Figure 4:Hematoxylin and eosin-stained section at ×40 magnification (high power) shows the cellular morphology. The cells have round to oval hyperchromatic nuclei with prominent nucleoli and scant cytoplasm. Mitotic activity is brisk
| Figure 5:Immunohistochemistry: CD 20-strong diffuse membrane positivity in round cells
| Figure 6:CT scan post six cycles of R-CHOP showing complete resolution of the disease
References
- Dimopoulos MA, Daliani D, Pugh W, Gershenson D, Cabanillas F, Sarris AH. Primary ovarian non-Hodgkin′s lymphoma: Outcome after treatment with combination chemotherapy. Gynecol Oncol 1997;64:446-50.
- Osborne BM, Robboy SJ. Lymphomas or leukemia presenting as ovarian tumors. An analysis of 42 cases. Cancer 1983;52:1933-43.
- Lagoo AS, Robboy SJ. Lymphoma of the female genital tract: Current status. Int J Gynecol Pathol 2006;25:1-21.
- Kosari F, Daneshbod Y, Parwaresch R, Krams M, Wacker HH. Lymphomas of the female genital tract: A study of 186 cases and review of the literature. Am J Surg Pathol 2005;29:1512-20.
- Woodruff JD, NoliCastillord, Novak ER. Lymphoma of the ovary. A study of 35 cases from the Ovarian Tumor Registry of the American Gynecological Society. Am J Obstet Gynecol 1963;85:912-8.
- Hauswirth AW, Skrabs C, Schützinger C, Gaiger A, Lechner K, Jäger U. Autoimmune hemolytic anemias, Evans′ syndromes, and pure red cell aplasia in non-Hodgkin lymphomas. Leuk Lymphoma 2007;48:1139-49.
- Ambulkar I, Nair R. Primary ovarian lymphoma: Report of cases and review of literature. Leuk Lymphoma 2003;44:825-7.
- Monterroso V, Jaffe ES, Merino MJ, Medeiros LJ. Malignant lymphomas involving the ovary: A clinicopathologic analysis of 39 cases. Am J Surg Pathol 1993;17:154-70.
- Skodras G, Fields V, Kragel PJ. Ovarian lymphomas and serous carcinoma of low malignant potential arising in the same ovary: A case report with literature review of primary ovarian lymphoma. Arch Pathol Lab Med 1994;118:647-50.
- ;Ferry JA, Young RH. Malignant lymphomas, pseuso lymphomas and hematopoeitic disorders of the female genital tract. Pathol Ann 1991;26:227-63.
- ;Moreno C, Hodgson K, Ferrer G, Elena M, Filella X, Pereira A, et al. Autoimmune cytopenia in chronic lymphocytic leukemia: Prevalence, clinical associations, and prognostic significance. Blood 2010;116:4771-6.
- Eve HE, Rule SA. Autoimmune haemolyticanaemia associated with mantle cell lymphoma. Int J Hematol 2010;91:322-5.
- McKelvey EM, Gottlieb JA, Wilson HE, Haut A, Talley RW, Stephens R, et al. Hydroxyldaunomycin (Adriamycin) combination chemotherapy in malignant lymphoma. Cancer 1976;38:1484-93.
- Kim KM, Yoon DH, Lee SG, Lim SN, Sug LJ, Huh J, et al. A case of primary adrenal diffuse large B-cell lymphoma achieving complete remission with Rituximab -CHOP chemotherapy. J Korean Med Sci2009;24:525-8.
- Ferreri AJ, Dognini GP, Bairey O, Szomor A, Montalbán C, Horvath B, et al. The addition of rituximab to anthracycline-based chemotherapy significantly improves outcome in ′Western′ patients with intravascular large B-cell lymphoma. Br J Haematol 2008;143:253-7.
- Rajnics P, Demeter J, Csomor J, Krenács L, Pajor L, Kollár B, et al. Rare primary extranodal lymphomas: Diffuse large B-cell lymphomas of the genital tract. Ann Hematol 2009;88:1223-8.
- Komoto D, Nishiyama Y, Yamamoto Y, Monden T, Sasakawa Y, Toyama Y, et al. A case of non-Hodgkin′s lymphoma of the ovary: Usefulness of 18F-FDG PET for staging and assessment of the therapeutic response. Ann Nucl Med 2006;20:157-60.
- Signorelli M, Maneo A, Cammarota S, Isimbaldi G, Garcia Parra R, Perego P, et al. Conservative management in primary genital lymphomas: The role of chemotherapy. Gynecol Oncol 2007;104:416-21.
- Yun J, Kim SJ, Won JH, Choi CW, Eom HS, Kim JS, et al. Clinical features and prognostic relevance of ovarian involvement in non-Hodgkin′s lymphoma: A consortium for improving survival of lymphoma (CISL) report. Leuk Res 2010;34:1175-9.
- Peñalver FJ, Alvarez-Larrán A, Díez-Martin JL, Gallur L, Jarque I, Caballero D, et al. Rituximab is an effective and safe therapeutic alternative in adults with refractory and severe autoimmune hemolytic anemia. Ann Hematol 2010;89:1073-80.
- Kaufman M, Limaye SA, Driscoll N, Johnson C, Caramanica A, Lebowicz Y, et al. A combination of rituximab, cyclophosphamide and dexamethasone effectively treats immune cytopenias of chronic lymphocytic leukemia. Leuk Lymphoma 2009;50:892-9.
- Gupta V, Shukla J, Bhatia BD. Autoimmune hemolytic anemia. Indian J Pediatr 2008;75:451-4.