 PDF
PDF  Views
Views  Share
Share


A Novel Presentation of Cutaneous Angiosarcoma: A Case Report and Review
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2017; 38(03): 363-366
DOI: DOI: 10.4103/ijmpo.ijmpo_81_16
Abstract
We report a case of a 70-year-old male, with slowly widening induration, ulceration, and oozing for 3 months on the scalp and face. The diagnosis of aggressive cutaneous angiosarcoma was made on histopathology and immunochemistry from the biopsy material from the involved area of the skin.
Publication History
Article published online:
04 July 2021
© 2017. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Abstract
We report a case of a 70-year-old male, with slowly widening induration, ulceration, and oozing for 3 months on the scalp and face. The diagnosis of aggressive cutaneous angiosarcoma was made on histopathology and immunochemistry from the biopsy material from the involved area of the skin.
Introduction
Cutaneous angiosarcoma is a rare soft tissue tumor found more often in the head and neck region. Less than 5%-cases of soft tissue sarcomas involve head and neck, 10%-of which are angiosarcomas.[1] They may present as single or multiple bluish or violaceous nodules or plaques or flat infiltrating areas which occasionally bleed or ulcerate.[2] They are known to be great mimickers and may mimic rosacea, local bruise, eczema, Kaposi sarcoma, and scarring alopecia to elucidate a few. This leads to wider extension and delay in diagnosis. We report a case of cutaneous angiosarcoma with unsuspecting presentation and rarity.
Case Report
A 70-year-old male presented with progressively extending, mildly painful, ulcerated, and red indurated skin lesion involving the left side of the scalp for 3 months and the face for 10 days. Three months back, he noticed a painless swelling with oozing on the left side of the vertex of the scalp. This slowly spread into surrounding tissue. Some of the area ulcerated and black eschar formed over it. The mild ooze continued and the surrounding peripheral skin hardened and progressed to involve the left side of the forehead, the periorbital region, and the upper left cheek. Besides, he had been unable to open his left eye for 10 days [Figure 1].

| Figure 1:Frontal view of an erythematous, indurated, stony hard plaque with central eschar on the scalp associated with edema of the left upper eyelid

| Figure 2:Lateral view of the same patient showing involvement of most of the left side of scalp, cheek, and pinna
His blood glucose was 145 mg/dl fasting and 280 mg/dl postprandial. Hemogram, renal and liver function tests were within normal limits. A provisional diagnosis of cellulitis with diabetes mellitus was kept and he was treated accordingly. The discharge sent for the culture revealed Acinetobacter. The treatment was changed as per the sensitivity profile. After initial improvement on antibiotics, the erythema and induration not only persisted but also progressed.
Fine-needle aspiration cytology from the left posterior cervical lymph nodes and left cheek revealed round to spindle-shaped cells, arranged in clusters with anisocytosis and coarse chromatin. They were probably malignant cells of mesenchymal origin along with acute inflammatory cells and necrosis.
Skin biopsy from the edge of the plaque in the scalp divulged ulcerated epidermis and a tumor in the dermis. The tumor cells were pleomorphic, and the nuclei were hyperchromatic, plump, and spindle-shaped. The cells with occasional mitosis were arranged in sheets and at places lined with irregular slit-like spaces, infiltrating into the surrounding collagenous stroma and arrector pili muscle [Figure 3]. No infiltration into the lymphatics or blood vessels could be detected. Immunohistochemistry done in the biopsied skin showed positive CD34, CD31, vascular endothelial growth factor (VEGF), and vimentin while pan cytokeratin was negative [Figure 4]. It was thus confirmed to be cutaneous angiosarcoma. X-ray chest was normal. X-ray and contrast-enhanced computed tomography (CECT) head and neck revealed no evidence of skull invasion or intracranial extension. Ultrasound abdomen and CECT chest and abdomen showed no systemic metastasis. The patient was referred to oncology department but succumbed in 6 months.
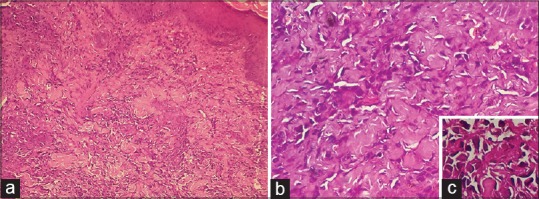
| Figure 3:(a) Histopathology slide showing skin biopsy specimen with tumor cells (H and E, ×100). (b and c) Pleomorphic, hyperchromatic, plump tumor cells with spindle-shaped nuclei in the dermis. Cells with occasional mitosis were arranged in sheets and at places lined with irregular slit-like spaces, infiltrating into surrounding collagenous stroma and arrector pili muscle (inset) (×400)

| Figure 4:Immunohistochemical stains show positive CD31, vascular endothelial growth factor, and vimentin and negative for pan cytokeratin
Discussion
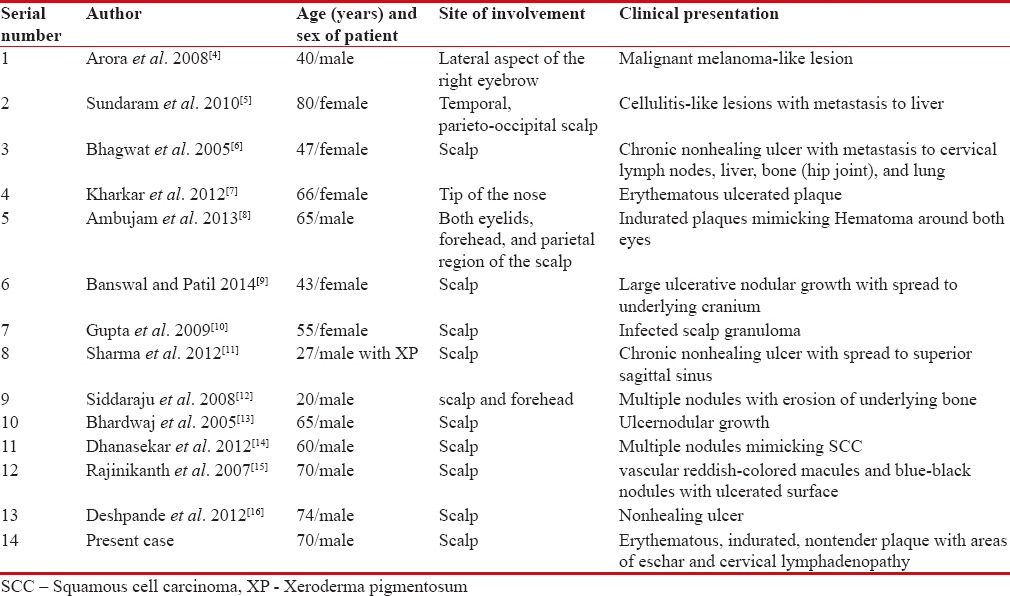
Angiosarcomas are rare malignant tumors derived from endothelial cells that line the blood vessels. They constitute only 1%–2%-of all soft tissue sarcomas while sarcomas themselves account for <-1% of all malignancies.[3] They can be either cutaneous or visceral involving the breast, spleen, and liver.[3] Scalp angiosarcoma usually occurs in elderly men in the seventh to eighth decade of life with an estimated male-to-female ratio of 3:1.[2] However, 14 cases (including the present case) reported from India have a male-to-female ratio of 1.8:1 and an early age of onset [Table 1].
Table 1
List of Indian cases published till date with their age, site, presentation, and prognosis
| Predisposing factors for angiosarcoma include trauma, chronic lymphedema, irradiation, and age. Due to its wide range of plausible etiologies, it has been categorized into lymphedema-associated, radiation-induced, primary breast angiosarcoma, sporadic cutaneous angiosarcoma (age related), commonly located on the head and neck region,[13] and angiosarcoma of the soft tissue.[17] Although chronic lymphedema is the most widely recognized predisposing factor in angiosarcoma of the skin and soft tissue, other common predisposing factors may be trauma, irradiation, and age per se.[17] Our case had a short clinical history of 3 months of stony hard progressively increasing plaque in the scalp with cervical lymphadenopathy. This only stands to reason that these findings suggest that lymphedema had occurred secondary to the infiltrating tumor mass rather than the tumor secondarily developing in lymphedema, as has been described earlier. The lymphedema in this case could either be due to compression or blockage of the lymphatics by the invading tumor mass.
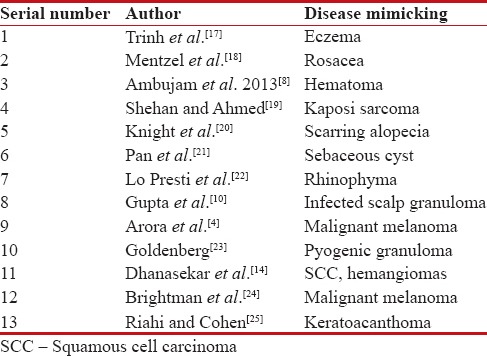
Cutaneous angiosarcomas are known to be great mimickers and may present as single or multiple, bluish or violaceous nodules, plaques, or flat infiltrating lesions.[2,17] Occasionally, they may ulcerate or bleed. They have often being described in literature to mimic rosacea,[18] local bruise,[8] eczema,[17] Kaposi sarcoma,[19] scarring alopecia,[20] sebaceous cysts,[21] and rhinophyma[22] and thus delaying the diagnosis [Table 2].
Table 2
List of conditions and clinical presentations cutaneous angiosarcoma has been reported to mimic
| Histologically, angiosarcomas often extensively involve the dermis, and the poorly differentiated tumors invade deep structures, such as fascia and subcutis. The histologic patterns in which it can occur are around vascular channels, sheets of cells, and cells with undifferentiated morphologic features. Low-grade angiosarcomas are well-differentiated lesions that retain some of the functional and morphologic properties of normal vascular endothelium. In high-grade tumors, cells are poorly differentiated and sheets of pleomorphic cells may resemble a carcinoma. They may have areas of hemorrhage, distorted architecture, and large cells with hyperchromatic, pleomorphic nuclei.[2,10] Immunohistochemical markers include von Willebrand factor, CD34, CD31, Ulex europaeus agglutinin 1, VEGF, and factor VIII antigen.[17] The most sensitive and specific marker for endothelial differentiation is CD31. Von Willebrand factor is fairly specific, and Ulex europaeus agglutinin has poor sensitivity and specificity, thus were not done.[3] In our case, besides, CD31+ cells and CD34+ cells, VEGF, and vimentin were also positive.
Angiosarcoma has a tendency for aggressive local as well as distant metastasis through lymphatic and hematogenous routes. The rate of regional nodal involvement is said to be 20%–30%, which is higher than most other sarcomas. The most common site for metastasis is lungs. Thin-walled, cystic pulmonary lesions and pneumothorax are characteristic findings.[2,3] Other less common sites of distant spread are liver, spleen, and bone. This case had metastasis to the lymph nodes while metastasis to other organs could not be detected. The overall prognosis for patients with angiosarcoma of the head and neck remains dismal, with a reported 5-year survival rate of approximately 10%–20%.[2,3] The delay in diagnosis due to initial misinterpretation, advanced age at presentation, lesions >5 cm in greatest dimension, multifocal nature of lesions at presentation, poor histological grade, lesions that initially cannot be surgically resected, and lesions with greater depth of invasion are the major factors responsible for poor prognosis reported in cutaneous angiosarcomas.[3,10]
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.[25]
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Aust MR, Olsen KD, Lewis JE, Nascimento AG, Meland NB, Foote RL, et al. Angiosarcomas of the head and neck: Clinical and pathologic characteristics. Ann Otol Rhinol Laryngol 1997;106:943-51.
- Pawlik TM, Paulino AF, McGinn CJ, Baker LH, Cohen DS, Morris JS, et al. Cutaneous angiosarcoma of the scalp: A multidisciplinary approach. Cancer 2003;98:1716-26.
- Barnett CR, Bakr FS, Grossman ME. Cutaneous angiosarcoma with skin metastases and persistent bloody pleural effusions. Cutis 2012;89:129-32.
- Arora R, Sharma A, Gupta R, Vijayaraghavan M. Cutaneous angiosarcoma in a patient with xeroderma pigmentosum. Indian J Pathol Microbiol 2008;51:504-6.
- Sundaram M, Vetrichevvel TP, Subramanyam S, Subramaniam A. Primary multicentric cutaneous epithelioid angiosarcoma. Indian J Dermatol Venereol Leprol 2011;77:111.
- Bhagwat R, Biswas G, Goyal L, Sastry P, Vora A, Parikh PM. Cutaneous angiosarcoma of the scalp. Indian J Med Paediatr Oncol 2005;26:51-2.
- Kharkar V, Jadhav P, Thakkar V, Mahajan S, Khopkar U. Primary cutaneous angiosarcoma of the nose. Indian J Dermatol Venereol Leprol 2012;78:496-7.
- Ambujam S, Audhya M, Reddy A, Roy S. Cutaneous angiosarcoma of the head, neck, and face of the elderly in type 5 skin. J Cutan Aesthet Surg 2013;6:45-7.
- Banswal L, Patil R. Rare case of recurrent angiosarcoma of the scalp: A case report and review of literature. Int Surg J 2014;1:33.
- Gupta MD, Chakrabarti N, Agrawal P, Narurkar S. Angiosarcoma of the scalp. Indian J Plast Surg 2009;42:118-21.
- Sharma S, Deshmukh AD, Bal MM, Chaukar DA, Dcruz AK. Angiosarcoma of the scalp associated with xeroderma pigmentosum. Indian J Med Paediatr Oncol 2012;33:126-9.
- Siddaraju N, Soundararaghavan J, Bundele MM, Roy SK. Fine needle aspiration cytology of epithelioid angiosarcoma: A case report. Acta Cytol 2008;52:109-13.
- Bhardwaj M, Gautam RK, Sharma PK, Kar HK, Magoon N, Sharma A. Angiosarcoma of scalp: A case report. Indian J Pathol Microbiol 2005;48:497-9.
- Dhanasekar P, Karthikeyan VS, Rajkumar N, Chandra Sistla S, Manwar Ali S, Basu D, et al. Cutaneous angiosarcoma of the scalp masquerading as a squamous cell carcinoma: Case report and literature review. J Cutan Med Surg 2012;16:187-90.
- Rajinikanth J, Gaikwad P, Raj JP, Tirkey AJ, Muthusami JC. Angiosarcoma of the scalp. Otolaryngol Head Neck Surg 2008;138:255-6.
- Deshpande DJ, Nayak CS, Mishra SN. A non healing ulcer on scalp. Acta Medica (Hradec Kralove) 2012;55:53-5.
- Trinh NQ, Rashed I, Hutchens KA, Go A, Melian E, Tung R. Unusual clinical presentation of cutaneous angiosarcoma masquerading as eczema: A case report and review of the literature. Case Rep Dermatol Med 2013;2013:906426.
- Mentzel T, Kutzner H, Wollina U. Cutaneous angiosarcoma of the face: Clinicopathologic and immunohistochemical study of a case resembling rosacea clinically. J Am Acad Dermatol 1998;38(5 Pt 2):837-40.
- Shehan JM, Ahmed I. Angiosarcoma arising in a lymphedematous abdominal pannus with histologic features reminiscent of Kaposi's sarcoma: Report of a case and review of the literature. Int J Dermatol 2006;45:499-503.
- Knight TE, Robinson HM Jr., Sina B. Angiosarcoma (angioendothelioma) of the scalp. An unusual case of scarring alopecia. Arch Dermatol 1980;116:683-6.
- Pan Z, Albertson D, Bhuller A, Wang B, Shehan JM, Sarma DP. Angiosarcoma of the scalp mimicking a sebaceous cyst. Dermatol Online J 2008;14:13.
- Lo Presti M, Mazzella C, Monfrecola A, Falleti J. Angiosarcoma mimicking rhinophyma. Dermatol Res Pract 2010;2010:365173.
- Goldenberg AS. The symptoms of an angiosarcoma mimicking pulpal pain. J Endod 1983;9:65-70.
- Brightman LA, Demierre MF, Byers HR. Macrophage-rich epithelioid angiosarcoma mimicking malignant melanoma. J Cutan Pathol 2006;33:38-42.
- Riahi RR, Cohen PR. Malignancies with skin lesions mimicking keratoacanthoma. Dermatol Online J 2013;19:20397.
| Figure 1:Frontal view of an erythematous, indurated, stony hard plaque with central eschar on the scalp associated with edema of the left upper eyelid
| Figure 2:Lateral view of the same patient showing involvement of most of the left side of scalp, cheek, and pinna
| Figure 3:(a) Histopathology slide showing skin biopsy specimen with tumor cells (H and E, ×100). (b and c) Pleomorphic, hyperchromatic, plump tumor cells with spindle-shaped nuclei in the dermis. Cells with occasional mitosis were arranged in sheets and at places lined with irregular slit-like spaces, infiltrating into surrounding collagenous stroma and arrector pili muscle (inset) (×400)
| Figure 4:Immunohistochemical stains show positive CD31, vascular endothelial growth factor, and vimentin and negative for pan cytokeratin
References
- Aust MR, Olsen KD, Lewis JE, Nascimento AG, Meland NB, Foote RL, et al. Angiosarcomas of the head and neck: Clinical and pathologic characteristics. Ann Otol Rhinol Laryngol 1997;106:943-51.
- Pawlik TM, Paulino AF, McGinn CJ, Baker LH, Cohen DS, Morris JS, et al. Cutaneous angiosarcoma of the scalp: A multidisciplinary approach. Cancer 2003;98:1716-26.
- Barnett CR, Bakr FS, Grossman ME. Cutaneous angiosarcoma with skin metastases and persistent bloody pleural effusions. Cutis 2012;89:129-32.
- Arora R, Sharma A, Gupta R, Vijayaraghavan M. Cutaneous angiosarcoma in a patient with xeroderma pigmentosum. Indian J Pathol Microbiol 2008;51:504-6.
- Sundaram M, Vetrichevvel TP, Subramanyam S, Subramaniam A. Primary multicentric cutaneous epithelioid angiosarcoma. Indian J Dermatol Venereol Leprol 2011;77:111.
- Bhagwat R, Biswas G, Goyal L, Sastry P, Vora A, Parikh PM. Cutaneous angiosarcoma of the scalp. Indian J Med Paediatr Oncol 2005;26:51-2.
- Kharkar V, Jadhav P, Thakkar V, Mahajan S, Khopkar U. Primary cutaneous angiosarcoma of the nose. Indian J Dermatol Venereol Leprol 2012;78:496-7.
- Ambujam S, Audhya M, Reddy A, Roy S. Cutaneous angiosarcoma of the head, neck, and face of the elderly in type 5 skin. J Cutan Aesthet Surg 2013;6:45-7.
- Banswal L, Patil R. Rare case of recurrent angiosarcoma of the scalp: A case report and review of literature. Int Surg J 2014;1:33.
- Gupta MD, Chakrabarti N, Agrawal P, Narurkar S. Angiosarcoma of the scalp. Indian J Plast Surg 2009;42:118-21.
- Sharma S, Deshmukh AD, Bal MM, Chaukar DA, Dcruz AK. Angiosarcoma of the scalp associated with xeroderma pigmentosum. Indian J Med Paediatr Oncol 2012;33:126-9.
- Siddaraju N, Soundararaghavan J, Bundele MM, Roy SK. Fine needle aspiration cytology of epithelioid angiosarcoma: A case report. Acta Cytol 2008;52:109-13.
- Bhardwaj M, Gautam RK, Sharma PK, Kar HK, Magoon N, Sharma A. Angiosarcoma of scalp: A case report. Indian J Pathol Microbiol 2005;48:497-9.
- Dhanasekar P, Karthikeyan VS, Rajkumar N, Chandra Sistla S, Manwar Ali S, Basu D, et al. Cutaneous angiosarcoma of the scalp masquerading as a squamous cell carcinoma: Case report and literature review. J Cutan Med Surg 2012;16:187-90.
- Rajinikanth J, Gaikwad P, Raj JP, Tirkey AJ, Muthusami JC. Angiosarcoma of the scalp. Otolaryngol Head Neck Surg 2008;138:255-6.
- Deshpande DJ, Nayak CS, Mishra SN. A non healing ulcer on scalp. Acta Medica (Hradec Kralove) 2012;55:53-5.
- Trinh NQ, Rashed I, Hutchens KA, Go A, Melian E, Tung R. Unusual clinical presentation of cutaneous angiosarcoma masquerading as eczema: A case report and review of the literature. Case Rep Dermatol Med 2013;2013:906426.
- Mentzel T, Kutzner H, Wollina U. Cutaneous angiosarcoma of the face: Clinicopathologic and immunohistochemical study of a case resembling rosacea clinically. J Am Acad Dermatol 1998;38(5 Pt 2):837-40.
- Shehan JM, Ahmed I. Angiosarcoma arising in a lymphedematous abdominal pannus with histologic features reminiscent of Kaposi's sarcoma: Report of a case and review of the literature. Int J Dermatol 2006;45:499-503.
- Knight TE, Robinson HM Jr., Sina B. Angiosarcoma (angioendothelioma) of the scalp. An unusual case of scarring alopecia. Arch Dermatol 1980;116:683-6.
- Pan Z, Albertson D, Bhuller A, Wang B, Shehan JM, Sarma DP. Angiosarcoma of the scalp mimicking a sebaceous cyst. Dermatol Online J 2008;14:13.
- Lo Presti M, Mazzella C, Monfrecola A, Falleti J. Angiosarcoma mimicking rhinophyma. Dermatol Res Pract 2010;2010:365173.
- Goldenberg AS. The symptoms of an angiosarcoma mimicking pulpal pain. J Endod 1983;9:65-70.
- Brightman LA, Demierre MF, Byers HR. Macrophage-rich epithelioid angiosarcoma mimicking malignant melanoma. J Cutan Pathol 2006;33:38-42.
- Riahi RR, Cohen PR. Malignancies with skin lesions mimicking keratoacanthoma. Dermatol Online J 2013;19:20397.