 PDF
PDF  Views
Views  Share
Share


Adenomatoid tumor of cervix: The first case report
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2016; 37(01): 66
DOI: DOI: 10.4103/0971-5851.177039

Publication History
Article published online:
12 July 2021
© 2016. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
A 32-year-old female presented with vague lower abdominal pain. Instant per speculum examination and pelvic ultrasound revealed a sessile polypoid mass projecting from the posterior cervical wall. No other clinico-radiologically distinguishable abdominopelvic pathology could be ratified. Polypectomy was performed soon after under regional anesthesia.
Grossly, the mass measured 2.3 cm × 2.2 cm × 2.2 cm. It was covered by glistening pearly white surface epithelium. Cut section exposed a well-defined, whitish, homogeneous mass. Its immaculate delineation from the surface was obvious, even at macroscopic inspection [Figure 1].
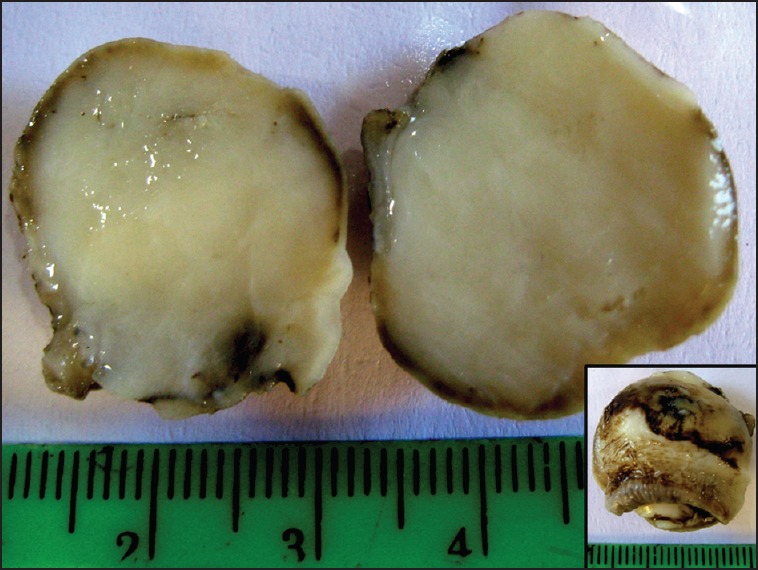
| Fig. 1 Adenomatoid tumor of cervix: Grossly, small globular mass with smooth glistening exterior surface (inset); cut surface is homogeneous, white and well-delineated from surface epithelium
Microscopically, the neoplasm was well-circumscribed and separated from its surface by a rim of fibroconnective tissue. It exhibited an array of architectural patterns: Tubuloglandular structures, microcysts, and solid sheets with focal lymphocytic infiltrates. The flattened-to-cuboidal neoplastic cells featured fine nuclear chromatin, inconspicuous nucleoli, and abundant vacuolated cytoplasm [Figure [Figure2A2A–C]. Nuclear pleomorphism or mitoses were absent. The overall histomorphology provisionally favored the diagnosis of “adenomatoid tumor” (AT), but differentials such as various endothelial/lipomatous neoplasms needed exclusion. The tumor cells expressed strong immunoreactivity for calretinin [Figure 2D]. Ultimately, it became the maiden case of cervical AT.
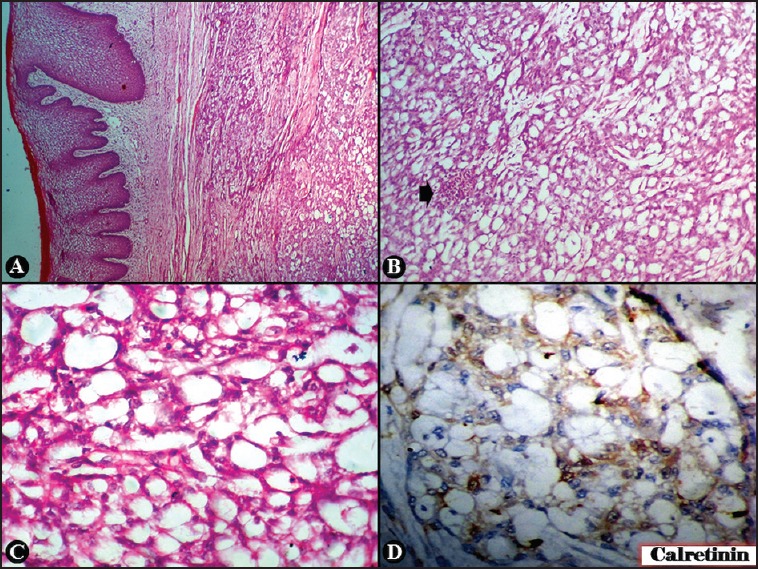
| Fig. 2 Adenomatoid tumor of cervix: Well-circumscribed mass separated from mucosa by a rim of fibroconnective tissue (H and E, ×40) (a). Neoplastic cells in sheets, tubules, microcysts, with focal (arrow) lymphocytic infiltration (H and E, ×100) (b); contain fine nuclear chromatin, inconspicuous nucleoli, and abundant vacuolated cytoplasm (H and E, ×400) (c). Cells positive for calretinin (×400) (d)
| Fig. 1 Adenomatoid tumor of cervix: Grossly, small globular mass with smooth glistening exterior surface (inset); cut surface is homogeneous, white and well-delineated from surface epithelium
| Fig. 2 Adenomatoid tumor of cervix: Well-circumscribed mass separated from mucosa by a rim of fibroconnective tissue (H and E, ×40) (a). Neoplastic cells in sheets, tubules, microcysts, with focal (arrow) lymphocytic infiltration (H and E, ×100) (b); contain fine nuclear chromatin, inconspicuous nucleoli, and abundant vacuolated cytoplasm (H and E, ×400) (c). Cells positive for calretinin (×400) (d)