 PDF
PDF  Views
Views  Share
Share


Cannonball Pulmonary Metastases in Gallbladder Cancer
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2017; 38(01): 93-94
DOI: DOI: 10.4103/0971-5851.203506
|
Publication History
Article published online:
06 July 2021
© 2017. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Sir,
A 25-year-old woman, nondiabetic and normotensive, presented with deep jaundice, weakness, and fatigue for the last 1 month. She had been asymptomatic before this. She gave a history of pruritus that had rapidly progressed over the last 1 month. Over the last 10 days, she had developed dry cough and dyspnea. She had no history of fever, hemoptysis, or pain abdomen.
Physical examination revealed mild pallor and severe jaundice. No lymph nodes were palpable, but chest examination revealed bilateral diffuse crepitations.
Routine blood tests revealed hemoglobin 7.8 g/dL, bilirubin 10.7 g/dL (direct: 8.2 g/dL, indirect fraction: 2.5 g/dL), aspartate aminotransferase – 68 U/L, alanine aminotransferase – 70 U/L, and alkaline phosphatase – 780 U/L. Viral serology for hepatitis A, B, C, and E was negative.
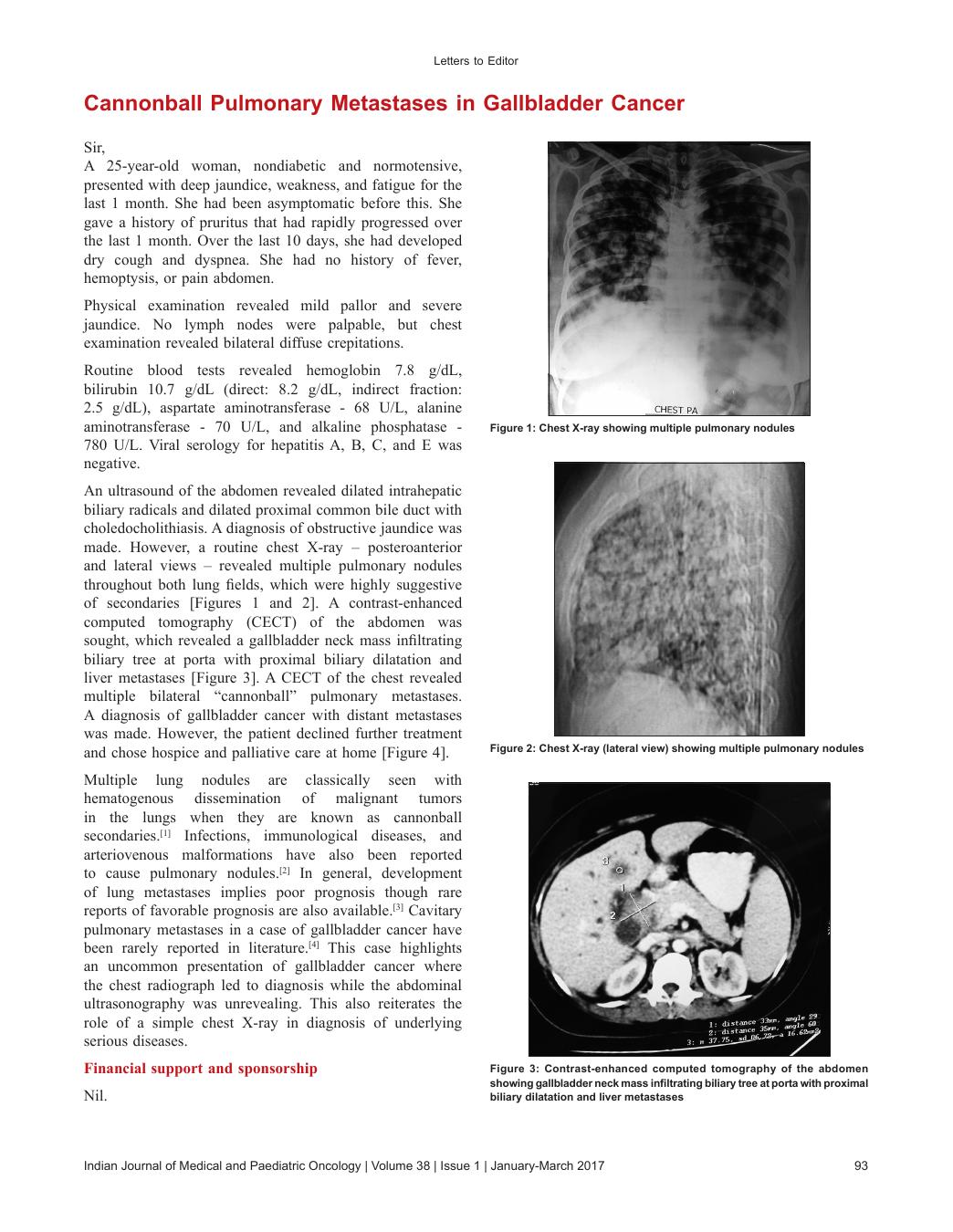
An ultrasound of the abdomen revealed dilated intrahepatic biliary radicals and dilated proximal common bile duct with choledocholithiasis. A diagnosis of obstructive jaundice was made. However, a routine chest X-ray – posteroanterior and lateral views – revealed multiple pulmonary nodules throughout both lung fields, which were highly suggestive of secondaries [Figures [Figures11 and and2].2]. A contrast-enhanced computed tomography (CECT) of the abdomen was sought, which revealed a gallbladder neck mass infiltrating biliary tree at porta with proximal biliary dilatation and liver metastases [Figure 3]. A CECT of the chest revealed multiple bilateral “cannonball” pulmonary metastases. A diagnosis of gallbladder cancer with distant metastases was made. However, the patient declined further treatment and chose hospice and palliative care at home [Figure 4].
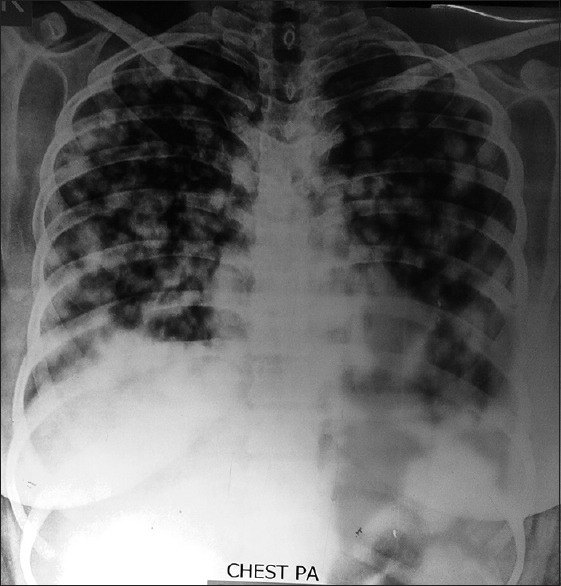
| Figure 1Chest X-ray showing multiple pulmonary nodules

| Figure 2Chest X-ray (lateral view) showing multiple pulmonary nodules
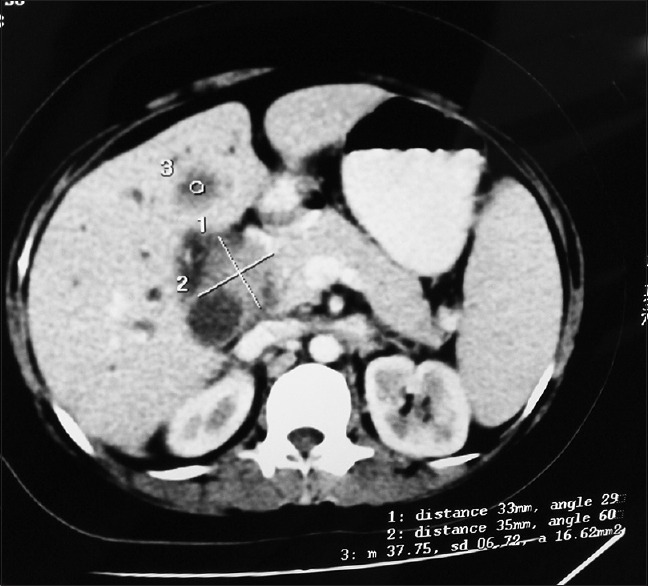
| Figure 3Contrast-enhanced computed tomography of the abdomen showing gallbladder neck mass infiltrating biliary tree at porta with proximal biliary dilatation and liver metastases
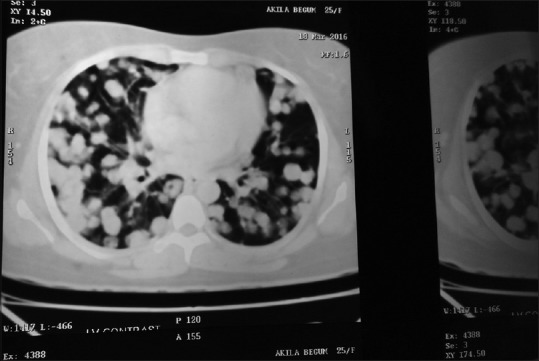
| Figure 4Contrast-enhanced computed tomography chest showing multiple bilateral “cannonball” pulmonary
Multiple lung nodules are classically seen with hematogenous dissemination of malignant tumors in the lungs when they are known as cannonball secondaries.[1] Infections, immunological diseases, and arteriovenous malformations have also been reported to cause pulmonary nodules.[2] In general, development of lung metastases implies poor prognosis though rare reports of favorable prognosis are also available.[3] Cavitary pulmonary metastases in a case of gallbladder cancer have been rarely reported in literature.[4] This case highlights an uncommon presentation of gallbladder cancer where the chest radiograph led to diagnosis while the abdominal ultrasonography was unrevealing. This also reiterates the role of a simple chest X-ray in diagnosis of underlying serious diseases.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Agarwal R, Mukhopadhyay J, Lahiri D, Biswas A, Maity P. Cannon-ball pulmonary metastases as a presenting feature of stomach cancer. Lung India 2015;32:300-2.
- Mohammed TL, Chowdhry A, Reddy GP, Amorosa JK, Brown K, Dyer DS, et al. ACR Appropriateness Criteria® screening for pulmonary metastases. J Thorac Imaging 2011;26:W1-3.
- Flavin R, Finn S, McErlean A, Smyth P, Meaney J, O'Connell F, et al. Cannonball metastases with favourable prognosis. Ir J Med Sci 2005;174:61-4.
- Baba K, Hattori T, Koishikawa I, Kamiya T, Noda A, Kobayashi T, et al. Cavitary pulmonary metastases of gallbladder cancer. Respiration 1998;65:219-22.
| Figure 1Chest X-ray showing multiple pulmonary nodules
| Figure 2Chest X-ray (lateral view) showing multiple pulmonary nodules
| Figure 3Contrast-enhanced computed tomography of the abdomen showing gallbladder neck mass infiltrating biliary tree at porta with proximal biliary dilatation and liver metastases
| Figure 4Contrast-enhanced computed tomography chest showing multiple bilateral “cannonball” pulmonary
References
- Agarwal R, Mukhopadhyay J, Lahiri D, Biswas A, Maity P. Cannon-ball pulmonary metastases as a presenting feature of stomach cancer. Lung India 2015;32:300-2.
- Mohammed TL, Chowdhry A, Reddy GP, Amorosa JK, Brown K, Dyer DS, et al. ACR Appropriateness Criteria® screening for pulmonary metastases. J Thorac Imaging 2011;26:W1-3.
- Flavin R, Finn S, McErlean A, Smyth P, Meaney J, O'Connell F, et al. Cannonball metastases with favourable prognosis. Ir J Med Sci 2005;174:61-4.
- Baba K, Hattori T, Koishikawa I, Kamiya T, Noda A, Kobayashi T, et al. Cavitary pulmonary metastases of gallbladder cancer. Respiration 1998;65:219-22.