 PDF
PDF  Views
Views  Share
Share


Carotid Artery Stenosis in Head and Neck Cancer Patients Treated with Radiotherapy
CC BY 4.0 · Indian J Med Paediatr Oncol 2025; 46(05): 468-474
DOI: DOI: 10.1055/s-0045-1805024
Abstract
Introduction
Radiotherapy (RT) is a crucial treatment modality for 80% of head and neck cancer (HNC) patients, often combined with surgery or chemotherapy, leading to a significant reduction in cancer-related mortality. However, as cancer survival rates increase, therapy-related complications also increase, impacting both mortality and morbidity. One such late complication is radiation-induced carotid artery stenosis (CAS), a condition associated with an increased risk of cerebrovascular events. Radiation-induced CAS is rarely studied, especially in the Indian population. Despite its potential severity, there is no standardized screening or management protocol for radiation-induced CAS in HNC patients.
Objectives
This study aims to assess the prevalence, risk factors, complications, management, and outcomes of CAS in HNC patients who received RT, with or without chemotherapy and surgery at our institution.
Materials and Methods
This is a retrospective observational study of newly diagnosed primary HNC patients who received RT between January 2012 and December 2021. Patients with metastatic HNC and those treated elsewhere were excluded. Data on demographics, tumor characteristics, treatment, and imaging for vascular stenosis were collected. Statistical analysis was performed using R version 4.4.1, with categorical variables analyzed using the chi-square or Fisher's exact test and continuous variables using the Mann–Whitney's U test. Significance was set at p-value </= 0.05.
Results
Of 949 patients, 34 (3.6%) developed CAS. Preradiation vascular stenosis was rare (0.1%). Among the 34 patients categorized by time since treatment, CAS developed in 47.1% of patients after 5 years, 32.4% within 2 to 5 years, and 5.9% within 1 year. CAS severity included near-total occlusion in 23.5%, ≥70% stenosis in 20.6%, and neurological deficits in 8.8%. The median age was 62 years, and the majority were male (85.3%). Common risk factors were hypertension (29.4%), diabetes (20.6%), tobacco use (82.4%), and alcohol consumption (41.2%). Tumors of oral cavity and hypopharynx were more common. Most CAS patients (76.5%) received radical chemoradiation. Only 23.3% of CAS patients received anticoagulation therapy, with 14.3% undergoing mechanical thrombectomy.
Conclusion
This study highlights the prevalence of radiation-induced CAS in HNC patients, especially in the Indian population, and identifies associated risk factors. Hence, standardized screening and management protocols for CAS are crucial for improving long-term outcomes in HNC survivors.
Patient Consent
The patient consent was waived by the Institutional Ethics Committee.
Authors' Contribution
M.N. conceptualized the study and he is the guarantor. R.B. designed the study, defined the intellectual content, and edited the manuscript. R.B. and D.S. performed the literature search and prepared the manuscript. D.S. helped in data acquisition. J.M. performed the data analysis and statistical analysis. R.B. and M.N. reviewed the manuscript.
Publication History
Article published online:
03 March 2025
© 2025. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
- Stenting for Prevention of Carotid Blowout Syndrome in High-Risk Head and Neck Cancer PatientsBradley Kolb, Journal of Neurological Surgery Part B: Skull Base, 2020
- Stenting for Prevention of Carotid Blowout Syndrome in High-Risk Head and Neck Cancer PatientsBradley Kolb, VCOT Open, 2020
- Intervening in the Acute Phase of Postradiation Carotid Blowout SyndromeMarrigje A. de Jong, International Archives of Otorhinolaryngology, 2019
- Ocular Ischemic Syndrome: The Red Eye RevisitedSathya Narayanan, Journal of Clinical Interventional Radiology ISVIR
- Ocular Ischemic Syndrome: The Red Eye RevisitedSathya Narayanan, VCOT Open
- WALL SHEAR STRESS AND OSCILLATORY SHEAR INDEX DISTRIBUTION IN CAROTID ARTERY WITH VARYING DEGREE OF STENOSIS: A HEMODYNAMIC STUDY<svg viewBox="0 0 24 24" fill="none" xmlns="http://www.w3.org/2000/svg">
- MODELING AND HEMODYNAMIC SIMULATION OF HUMAN ARTERIAL STENOSIS VIA TRANSMISSION LINE MODEL<svg viewBox="0 0 24 24" fill="none" xmlns="http://www.w3.org/2000/svg">
- STRESS ANALYSIS OF INTERNAL CAROTID ARTERY WITH LOW STENOSIS LEVEL: THE EFFECT OF MATERIAL MODEL AND PLAQUE GEOMETRY<svg viewBox="0 0 24 24" fill="none" xmlns="http://www.w3.org/2000/svg">
- Streptococcus salivarius K12 Alleviates Oral Mucositis in Patients Undergoing Radiotherapy for Malignant Head and Neck Tumors: A Randomized Controlled Trial<svg viewBox="0 0 24 24" fill="none" xmlns="http://www.w3.org/2000/svg">
- DIAGNOSTIC AND THERAPEUTIC TREATMENTS OF PLAQUES IN THE CAROTID BIFURCATION — STUDIES IN MODELS WITH STENTS AND FILTERS<svg viewBox="0 0 24 24" fill="none" xmlns="http://www.w3.org/2000/svg">
Abstract
Introduction
Radiotherapy (RT) is a crucial treatment modality for 80%-of head and neck cancer (HNC) patients, often combined with surgery or chemotherapy, leading to a significant reduction in cancer-related mortality. However, as cancer survival rates increase, therapy-related complications also increase, impacting both mortality and morbidity. One such late complication is radiation-induced carotid artery stenosis (CAS), a condition associated with an increased risk of cerebrovascular events. Radiation-induced CAS is rarely studied, especially in the Indian population. Despite its potential severity, there is no standardized screening or management protocol for radiation-induced CAS in HNC patients.
Objectives
This study aims to assess the prevalence, risk factors, complications, management, and outcomes of CAS in HNC patients who received RT, with or without chemotherapy and surgery at our institution.
Materials and Methods
This is a retrospective observational study of newly diagnosed primary HNC patients who received RT between January 2012 and December 2021. Patients with metastatic HNC and those treated elsewhere were excluded. Data on demographics, tumor characteristics, treatment, and imaging for vascular stenosis were collected. Statistical analysis was performed using R version 4.4.1, with categorical variables analyzed using the chi-square or Fisher's exact test and continuous variables using the Mann–Whitney's U test. Significance was set at p-value <!--= 0.05.
Results
Of 949 patients, 34 (3.6%) developed CAS. Preradiation vascular stenosis was rare (0.1%). Among the 34 patients categorized by time since treatment, CAS developed in 47.1%-of patients after 5 years, 32.4%-within 2 to 5 years, and 5.9%-within 1 year. CAS severity included near-total occlusion in 23.5%, ≥70% stenosis in 20.6%, and neurological deficits in 8.8%. The median age was 62 years, and the majority were male (85.3%). Common risk factors were hypertension (29.4%), diabetes (20.6%), tobacco use (82.4%), and alcohol consumption (41.2%). Tumors of oral cavity and hypopharynx were more common. Most CAS patients (76.5%) received radical chemoradiation. Only 23.3%-of CAS patients received anticoagulation therapy, with 14.3%-undergoing mechanical thrombectomy.
Conclusion
This study highlights the prevalence of radiation-induced CAS in HNC patients, especially in the Indian population, and identifies associated risk factors. Hence, standardized screening and management protocols for CAS are crucial for improving long-term outcomes in HNC survivors.
Keywords
carotid artery stenosis - head and neck cancer - radiotherapy - cerebrovascular eventsIntroduction
Radiotherapy (RT) is an essential therapeutic modality in the treatment of 80%-of head and neck cancer (HNC) patients, often combined with surgery or chemotherapy. With the improvement in integrity of treatment, cancer-related mortality has been markedly reduced.[1] Since the number of cancer survivors has increased, therapy-related complications also increased, which impacted both mortality and morbidity.[2]
Among these complications, one of the underidentified and undertreated late complications is radiation-induced carotid artery stenosis (CAS), which is associated with a higher risk of cerebrovascular events.[3] Prevention and treatment of radiation-induced CAS is important for improving the long-term prognosis of the survivors.
Currently, there is no definitive algorithm for screening and subsequent management of CAS in HNC patients who have received radiation.[4] This study aims to analyze the prevalence, risk factors, and complications due to CAS in HNC patients treated with radiation, as well as its management and outcomes in our institution.
Materials and Methods
Study Design
This is a retrospective observational study.
Sample Size
Assuming an actuarial risk of 29%-for CAS at 8 years, as reported by Carpenter et al, the study required a minimum sample size of 317 participants. This sample size was calculated to estimate the expected proportion with an absolute precision of 5%-and a 95%-confidence interval. The calculation was performed using the Statulator's online sample size calculator.
All newly diagnosed primary patients with HNC who underwent RT ± chemotherapy and surgery from January 2012 to December 2021 were included in the study. Those patients with metastatic HNC, patients who defaulted treatment with radiation and patients with other synchronous malignancies and who had treatment elsewhere were excluded from the study. The demographic details of the study population, tumor characteristics, and treatment received were collected from the hospital-based registry medical records. The imaging modality used for diagnosis of vascular stenosis, the degree of stenosis, details of further evaluation, and management were reviewed in the study.
Primary Outcome: To analyze the incidence of CAS in HNC patients treated with radiation in our institution.
Secondary Outcome: To analyze the risk factors and complications due to CAS in HNC patients treated with radiation, as well as its management and outcomes.
Inclusion Criteria
Patients with HNC.
Biopsy-proven malignancies.
Patients who received treatment with radiation either alone or in combination with surgery or chemotherapy.
Patients above 18 years of age.
Exclusion Criteria
Patients with metastatic HNC.
Patients with other synchronous malignancies.
Statistical Analysis
Descriptive analysis was performed by mean, standard deviation, median, and interquartile range for continuous variables, and frequency and percentage for categorical variables. The significance of differences in the distribution of categorical variables among patients who developed vascular stenosis and who did not, such as diagnosis, subsites, and stages, was analyzed using the ci-square test and Fisher's exact test. The difference in the distribution of continuous variables was compared using the Mann–Whitney's U test for skewed distribution. Two-tailed significance at <0>
Ethical Approval
All the procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional or regional) and with the Declaration of Helsinki of 1975, as revised in 2013. This study was approved by the institutional ethics committee (G. Kuppuswamy Naidu Memorial Hospital), and patient informed consent for this study was waived as this is a retrospective study (ECR number 2023/IEC/059 dated December 21, 2023).
Results
Out of 949 patients, 34 of them had developed CAS. In the diagnostic evaluation of CAS among the subset of 34 patients, computed tomography (CT) imaging was the exclusive modality utilized. The analysis of preradiation vascular stenosis among the study cohort highlights a low prevalence (0.1%) of preexisting stenosis. Among the 34 patients categorized by time since treatment, 47.1%-developed CAS after 5 years of radiation, while 32.4%-within 2 to 5 years, 14.7%-within 1 to 2 years, and 5.9%-within 1 year postradiation ([Fig. 1]). The cumulative hazard rate at 5 years (60 months) is 0.0546 (confidence interval: 0.0333–0.0898) as compared with 10 years (120 months) of 0.3013 (confidence interval: 0.1736–0.5233). This signifies the cumulative hazard rate increases manyfold with time. Among 34 patients diagnosed with post-RT CAS, 23.5%-had near-total occlusion, 20.6%-had >/= 70%-stenosis, 17.6 had 40 to 50%-stenosis, and 8.8%- experienced neurological deficits (disorientation, giddiness, and paraplegia) attributed to the stenosis.

| Fig 1 : Showing the number of events (carotid artery stenosis) over a period of time.
The median age for those who developed stenosis was 62 (range 57–67.5). Among the 34 patients who developed CAS, 85.3%-were males and 14.7%-were females. Notably, individuals with stenosis demonstrated higher prevalence rates of hypertension (29.4%) and diabetes mellitus (20.6%). Coronary artery disease (CAD) was present in 5.9%-of patients, along with dyslipidemia (2.9%) and a history of cerebrovascular accident (CVA) (2.9%), compared with the general patient population. Other risk factors for atherosclerosis also need to be monitored. In patients with CAS, there was a higher prevalence of tobacco use (82.4%) and alcohol consumption (41.2%) compared with the total patient cohort. Conversely, a smaller proportion of those with stenosis reported no habits (17.6%).
Among 34 patients who developed CAS, the distribution of primary tumor was 29.4%-in the oral cavity, 29.4%-in the hypopharynx, 26.5%-in the oropharynx, 11.8%-in the larynx, and 2.9% in the nasopharynx.
Among patients who developed CAS, 44.1%-of them were in stage IV, 41.2%-in stage III, 11.8%-in stage II, and only 2.9%-in stage I ([Table 1]).
|
Characteristics (N = 949) |
N (%) |
Post-RT vascular stenosis |
p-Value[a] |
||
|---|---|---|---|---|---|
|
Yes (%) |
N (%) |
||||
|
949 |
34 (3.6%) |
915 (96.4%) |
|||
|
Age (y) |
Median (Q1, Q3) |
60 (51, 68) |
62 (57.2, 67.8) |
60 (50, 68) |
0.12[b] |
|
Sex |
Male |
746 (78.6%) |
29 (85.3%) |
717 (78.4%) |
|
|
Female |
203 (21.4%) |
5 (14.7%) |
198 (21.6%) |
0.45[c] |
|
|
Comorbidities |
HTN |
117 (12.3%) |
10 (29.4%) |
107 (11.7%) |
0.005 |
|
DM |
122 (12.9%) |
7 (20.6%) |
115 (12.6%) |
0.187 |
|
|
CAD |
34 (3.6%) |
2 (5.9%) |
32 (3.5%) |
0.346 |
|
|
DLP |
6 (0.6%) |
1 (2.9%) |
5 (0.5%) |
0.197 |
|
|
CVA |
6 (0.6%) |
1 (2.9%) |
5 (0.5%) |
0.197 |
|
|
None |
748 (78.8%) |
21 (61.8%) |
727 (79.5%) |
0.023[c] |
|
|
Habits |
Tobacco |
644 (67.9%) |
28 (82.4%) |
616 (67.3%) |
0.098[c] |
|
Alcohol |
249 (26.2%) |
14 (41.2%) |
235 (25.7%) |
0.069[c] |
|
|
None |
292 (30.8%) |
6 (17.6%) |
286 (31.3%) |
0.134[c] |
|
|
Diagnosis |
Ca oral cavity |
331 (34.9%) |
10 (29.4%) |
321 (35.1%) |
0.618[c] |
|
Ca hypopharynx |
222 (23.4%) |
10 (29.4%) |
212 (23.2%) |
0.523[c] |
|
|
Ca oropharynx |
209 (22%) |
9 (26.5%) |
200 (21.9%) |
0.67[c] |
|
|
Ca larynx |
120 (12.6%) |
4 (11.8%) |
116 (12.7%) |
1 |
|
|
Ca nasopharynx |
22 (2.3%) |
1 (2.9%) |
21 (2.3%) |
0.556 |
|
|
Others |
45 (4.7%) |
0 |
45 (4.9%) |
0.401 |
|
|
Stage |
I |
74 (7.8%) |
1 (2.9%) |
73 (8%) |
|
|
II |
275 (29%) |
4 (11.8%) |
271 (29.6%) |
||
|
III |
276 (29.1%) |
14 (41.2%) |
262 (28.6%) |
||
|
IV |
319 (33.6%) |
15 (44.1%) |
304 (33.2%) |
||
|
Preradiation vascular stenosis |
Yes |
1 (0.1%) |
0 |
1 (0.1%) |
|
|
No |
948 (99.9%) |
34 (100%) |
914 (99.9%) |
1 |
|
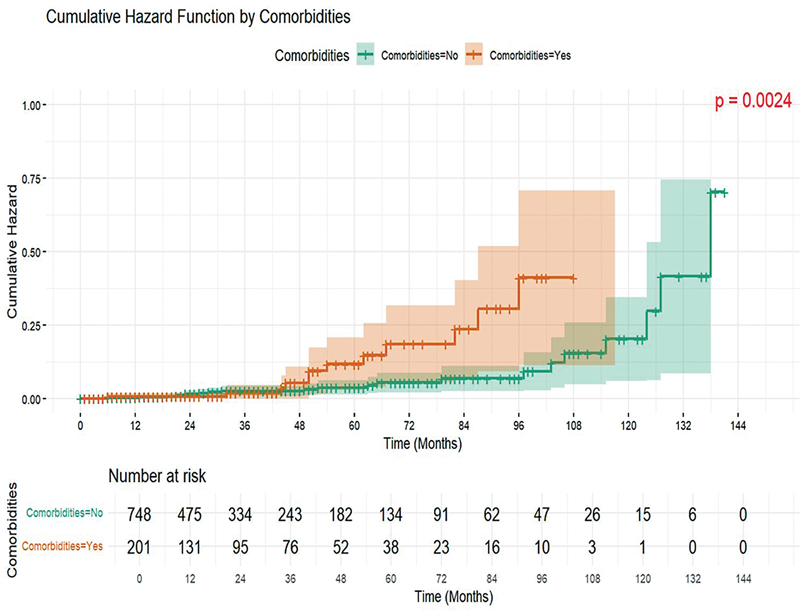
| Figure 2: Probability of onset of carotid artery stenosis in the presence of comorbidities.
Using a multivariate hazard regression model, which includes sex, cancer stage, overall RT dose delivered, and presence of comorbidities, we found higher hazard rates for the male gender, presence of comorbidities, and stages III and IV of disease ([Table 2]).
|
Characteristics |
N (%) |
Univariable |
Multivariable |
|||||
|---|---|---|---|---|---|---|---|---|
|
Hazard rate |
95%-CI |
p-Value |
Hazard rate |
95%-CI |
p-Value |
|||
|
Sex |
Female |
203 (21.4) |
||||||
|
Male |
746 (78.6) |
2.03 |
0.76–5.41 |
0.157 |
2.38 |
0.81–6.99 |
0.116 |
|
|
Comorbidities |
No |
748 (78.8) |
||||||
|
Yes |
201 (21.2) |
2.89 |
1.41–5.91 |
0.004 |
2.70 |
1.28–5.70 |
0.009 |
|
|
Dose delivered |
61–65 Gy |
9 (0.9) |
||||||
|
66–70 Gy |
740 (78.0) |
0.24 |
0.03–1.82 |
0.169 |
0.23 |
0.03–1.79 |
0.158 |
|
|
<!--= 60 Gy |
200 (21.1) |
0.09 |
0.01–0.88 |
0.039 |
0.08 |
0.01–0.88 |
0.038 |
|
|
Stage |
I |
74 (7.8) |
||||||
|
II |
275 (29.0) |
1.05 |
0.12–9.42 |
0.967 |
1.32 |
0.14–12.21 |
0.805 |
|
|
III |
276 (29.1) |
4.46 |
0.58–34.08 |
0.150 |
6.28 |
0.80–49.38 |
0.081 |
|
|
IV |
319 (33.6) |
6.21 |
0.82–47.25 |
0.078 |
7.07 |
0.91–54.78 |
0.061 |
|
|
Recurrence |
5 (0.5) |
0.00 |
0.00–infinity |
0.998 |
0.00 |
0.00–infinity |
0.998 |
|
References
-
Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019. CA Cancer J Clin 2019; 69 (01) 7-34
- Zhou M, Wang H, Zeng X. et al. Mortality, morbidity, and risk factors in China and its provinces, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 2019; 394 (10204): 1145-1158
- Lin PY, Cheng PC, Hsu WL. et al. Risk of CVD following radiotherapy for head and neck cancer: an updated systematic review and meta-analysis. Front Oncol 2022; 12: 820808
- Wagner AE, Goodman JS, Mitchell BJ. et al. Carotid artery stenosis in patients treated for head and neck cancer: a community based retrospective analysis. Clin Oncol Res 2018; (01) 1-4
- Thalhammer C, Husmann M, Glanzmann C, Studer G, Amann-Vesti BR. Carotid artery disease after head and neck radiotherapy. Vasa 2015; 44 (01) 23-30
- Xu J, Cao Y. Radiation-induced carotid artery stenosis: a comprehensive review of the literature. Intervent Neurol 2014; 2 (04) 183-192
- de Weerd M, Greving JP, de Jong AWF, Buskens E, Bots ML. Prevalence of asymptomatic carotid artery stenosis according to age and sex: systematic review and metaregression analysis. Stroke 2009; 40 (04) 1105-1113
- Kuo DY, Wu YW, Hsieh CH, Liao LJ, Shueng PW. Application of carotid duplex ultrasonography in the surveillance of carotid artery stenosis after neck irradiation. Rev Cardiovasc Med 2022; 23 (07) 240
- Messas E, Goudot G, Halliday A. et al. Management of carotid stenosis for primary and secondary prevention of stroke: state-of-the-art 2020: a critical review. Eur Heart J suppl 2020; 22 (suppl M): M35-M42
- Carpenter DJ, Mowery YM, Broadwater G. et al. The risk of carotid stenosis in head and neck cancer patients after radiation therapy. Oral Oncol 2018; 80: 9-15
- Cheng SW, Ting AC, Lam LK, Wei WI. Carotid stenosis after radiotherapy for nasopharyngeal carcinoma. Arch Otolaryngol Head Neck Surg 2000; 126 (04) 517-521
- Eckstein HH, Kühnl A, Dörfler A, Kopp IB, Lawall H, Ringleb PA. Multidisciplinary German-Austrian guideline based on evidence and consensus. The diagnosis, treatment and follow-up of extracranial carotid stenosis. Dtsch Arztebl Int 2013; 110 (27-28): 468-476
- Chang YJ, Chang TC, Lee TH, Ryu SJ. Predictors of carotid artery stenosis after radiotherapy for head and neck cancers. J Vasc Surg 2009; 50 (02) 280-285
- Lam WW, Leung SF, So NM. et al. Incidence of carotid stenosis in nasopharyngeal carcinoma patients after radiotherapy. Cancer 2001; 92 (09) 2357-2363
- Cheng YW, Chen CH, Yeh SJ. et al. Association between modifiable vascular risk factors and rapid progression of postradiation carotid artery stenosis. J Chin Med Assoc 2023; 86 (07) 627-632
- Dorth JA, Patel PR, Broadwater G, Brizel DM. Incidence and risk factors of significant carotid artery stenosis in asymptomatic survivors of head and neck cancer after radiotherapy. Head Neck 2014; 36 (02) 215-219
- Makita C, Okada S, Kajiura Y. et al. Vascular events from carotid artery atherosclerosis after radiation therapy for laryngeal and hypopharyngeal cancer: the incidence and risk factors. Nagoya J Med Sci 2020; 82 (04) 747-761
- Cheng SW, Wu LL, Ting AC, Lau H, Lam LK, Wei WI. Irradiation-induced extracranial carotid stenosis in patients with head and neck malignancies. Am J Surg 1999; 178 (04) 323-328
- Halak M, Fajer S, Ben-Meir H, Loberman Z, Weller B, Karmeli R. Neck irradiation: a risk factor for occlusive carotid artery disease. Eur J Vasc Endovasc Surg 2002; 23 (04) 299-302
- Zheng Z, Zhao Q, Wei J. et al. Medical prevention and treatment of radiation-induced carotid injury. Biomed Pharmacother 2020; 131: 110664
Address for correspondence
Publication History
Article published online:
03 March 2025
© 2025. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
- Stenting for Prevention of Carotid Blowout Syndrome in High-Risk Head and Neck Cancer PatientsBradley Kolb, Journal of Neurological Surgery Part B: Skull Base, 2020
- Stenting for Prevention of Carotid Blowout Syndrome in High-Risk Head and Neck Cancer PatientsBradley Kolb, VCOT Open, 2020
- Intervening in the Acute Phase of Postradiation Carotid Blowout SyndromeMarrigje A. de Jong, International Archives of Otorhinolaryngology, 2019
- Ocular Ischemic Syndrome: The Red Eye RevisitedSathya Narayanan, Journal of Clinical Interventional Radiology ISVIR
- Ocular Ischemic Syndrome: The Red Eye RevisitedSathya Narayanan, VCOT Open
- Mechanisms of Taste Bud Cell Loss after Head and Neck Irradiation<svg viewBox="0 0 24 24" fill="none" xmlns="http://www.w3.org/2000/svg">
- WALL SHEAR STRESS AND OSCILLATORY SHEAR INDEX DISTRIBUTION IN CAROTID ARTERY WITH VARYING DEGREE OF STENOSIS: A HEMODYNAMIC STUDY<svg viewBox="0 0 24 24" fill="none" xmlns="http://www.w3.org/2000/svg">
- MODELING AND HEMODYNAMIC SIMULATION OF HUMAN ARTERIAL STENOSIS VIA TRANSMISSION LINE MODEL<svg viewBox="0 0 24 24" fill="none" xmlns="http://www.w3.org/2000/svg">
- STRESS ANALYSIS OF INTERNAL CAROTID ARTERY WITH LOW STENOSIS LEVEL: THE EFFECT OF MATERIAL MODEL AND PLAQUE GEOMETRY<svg viewBox="0 0 24 24" fill="none" xmlns="http://www.w3.org/2000/svg">
- A novel needle mouse model of vascular cognitive impairment and dementia<svg viewBox="0 0 24 24" fill="none" xmlns="http://www.w3.org/2000/svg">
| Fig 1 : Showing the number of events (carotid artery stenosis) over a period of time.
| Figure 2: Probability of onset of carotid artery stenosis in the presence of comorbidities.
References
-
Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019. CA Cancer J Clin 2019; 69 (01) 7-34
- Zhou M, Wang H, Zeng X. et al. Mortality, morbidity, and risk factors in China and its provinces, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 2019; 394 (10204): 1145-1158
- Lin PY, Cheng PC, Hsu WL. et al. Risk of CVD following radiotherapy for head and neck cancer: an updated systematic review and meta-analysis. Front Oncol 2022; 12: 820808
- Wagner AE, Goodman JS, Mitchell BJ. et al. Carotid artery stenosis in patients treated for head and neck cancer: a community based retrospective analysis. Clin Oncol Res 2018; (01) 1-4
- Thalhammer C, Husmann M, Glanzmann C, Studer G, Amann-Vesti BR. Carotid artery disease after head and neck radiotherapy. Vasa 2015; 44 (01) 23-30
- Xu J, Cao Y. Radiation-induced carotid artery stenosis: a comprehensive review of the literature. Intervent Neurol 2014; 2 (04) 183-192
- de Weerd M, Greving JP, de Jong AWF, Buskens E, Bots ML. Prevalence of asymptomatic carotid artery stenosis according to age and sex: systematic review and metaregression analysis. Stroke 2009; 40 (04) 1105-1113
- Kuo DY, Wu YW, Hsieh CH, Liao LJ, Shueng PW. Application of carotid duplex ultrasonography in the surveillance of carotid artery stenosis after neck irradiation. Rev Cardiovasc Med 2022; 23 (07) 240
- Messas E, Goudot G, Halliday A. et al. Management of carotid stenosis for primary and secondary prevention of stroke: state-of-the-art 2020: a critical review. Eur Heart J suppl 2020; 22 (suppl M): M35-M42
- Carpenter DJ, Mowery YM, Broadwater G. et al. The risk of carotid stenosis in head and neck cancer patients after radiation therapy. Oral Oncol 2018; 80: 9-15
- Cheng SW, Ting AC, Lam LK, Wei WI. Carotid stenosis after radiotherapy for nasopharyngeal carcinoma. Arch Otolaryngol Head Neck Surg 2000; 126 (04) 517-521
- Eckstein HH, Kühnl A, Dörfler A, Kopp IB, Lawall H, Ringleb PA. Multidisciplinary German-Austrian guideline based on evidence and consensus. The diagnosis, treatment and follow-up of extracranial carotid stenosis. Dtsch Arztebl Int 2013; 110 (27-28): 468-476
- Chang YJ, Chang TC, Lee TH, Ryu SJ. Predictors of carotid artery stenosis after radiotherapy for head and neck cancers. J Vasc Surg 2009; 50 (02) 280-285
- Lam WW, Leung SF, So NM. et al. Incidence of carotid stenosis in nasopharyngeal carcinoma patients after radiotherapy. Cancer 2001; 92 (09) 2357-2363
- Cheng YW, Chen CH, Yeh SJ. et al. Association between modifiable vascular risk factors and rapid progression of postradiation carotid artery stenosis. J Chin Med Assoc 2023; 86 (07) 627-632
- Dorth JA, Patel PR, Broadwater G, Brizel DM. Incidence and risk factors of significant carotid artery stenosis in asymptomatic survivors of head and neck cancer after radiotherapy. Head Neck 2014; 36 (02) 215-219
- Makita C, Okada S, Kajiura Y. et al. Vascular events from carotid artery atherosclerosis after radiation therapy for laryngeal and hypopharyngeal cancer: the incidence and risk factors. Nagoya J Med Sci 2020; 82 (04) 747-761
- Cheng SW, Wu LL, Ting AC, Lau H, Lam LK, Wei WI. Irradiation-induced extracranial carotid stenosis in patients with head and neck malignancies. Am J Surg 1999; 178 (04) 323-328
- Halak M, Fajer S, Ben-Meir H, Loberman Z, Weller B, Karmeli R. Neck irradiation: a risk factor for occlusive carotid artery disease. Eur J Vasc Endovasc Surg 2002; 23 (04) 299-302
- Zheng Z, Zhao Q, Wei J. et al. Medical prevention and treatment of radiation-induced carotid injury. Biomed Pharmacother 2020; 131: 110664