 PDF
PDF  Views
Views  Share
Share


Cisplatin induced paroxysmal supraventricular tachycardia
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2013; 34(04): 330-332
DOI: DOI: 10.4103/0971-5851.125262
Abstract
Cisplatin or cis-diamminedichloroplatinum (CDDP) is the first member of a class of platinum-containing anti-cancer drugs that act by binding to and causing cross-linking of deoxyribonucleic acid, which ultimately triggers apoptosis. Cisplatin has a broad-spectrum antineoplastic activity against various types of human tumors. Unfortunately, the optimal usefulness of Cisplatin is limited secondary to its dose related toxicity especially nephrotoxicity. Cisplatin chemotherapy is also associated with cardiotoxic effects that may range from silent arrhythmias to heart failure and even sudden cardiac death. These effects are more pronounced when cisplatin is combined with other cardiotoxic drugs. Here, we report a case of patient of cancer lung who developed paroxysmal supraventricular tachycardia following administration of Cisplatin. A brief review of the literature follows.
Publication History
Article published online:
19 July 2021
© 2013. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Abstract
Cisplatin or cis-diamminedichloroplatinum (CDDP) is the first member of a class of platinum-containing anti-cancer drugs that act by binding to and causing cross-linking of deoxyribonucleic acid, which ultimately triggers apoptosis. Cisplatin has a broad-spectrum antineoplastic activity against various types of human tumors. Unfortunately, the optimal usefulness of Cisplatin is limited secondary to its dose related toxicity especially nephrotoxicity. Cisplatin chemotherapy is also associated with cardiotoxic effects that may range from silent arrhythmias to heart failure and even sudden cardiac death. These effects are more pronounced when cisplatin is combined with other cardiotoxic drugs. Here, we report a case of patient of cancer lung who developed paroxysmal supraventricular tachycardia following administration of Cisplatin. A brief review of the literature follows.
INTRODUCTION
Chemotherapy may induce entire spectrum of cardiac pathology. Cisplatin (CDDP) is a widely used chemotherapeutic agent and its use is limited by its wide range of toxicities, most common being renal and neurotoxicity. Cardiotoxicity of cisplatin is less common and may range from silent and symptomatic arrhythmias to cardiomyopathy and sudden death. Paroxysmal supraventricular tachycardia (PSVT) due to cisplatin is rare mentioned in only few case reports. We report a patient with no prior history of cardiac ailment who developed PSVT on administration of cisplatin that aborted once cisplatin was stopped.
CASE REPORT
Our patient was a 55-year-old male who had been recently diagnosed as having small cell carcinoma of the right lung. Patient was normotensive and had no underlying cardiac illness. Baseline electrocardiogram (ECG) and Echocardiography were normal as were other parameters [Figure 1a]. He was planned for cisplatin based chemotherapy Cisplatin (62 mg D1, D2 + Etoposide 165 mg D1, D2, D3). Patient received first cycle of chemotherapy uneventfully. During the second cycle while on cisplatin infusion, patient complained of palpitations. An ECG was performed that revealed PSVT [Figure 1b]. Cisplatin infusion was stopped and the patient was given diltiazem 15 mg intravenous. Meanwhile, blood samples were collected for serum Na+, K+, Ca2+ and Mg2+, which were reported as normal. Echocardiography and electrophysiological studies were carried out later, which were normal. Besides, subsequent ECGs were also normal [Figure 1c]. Patient received tab bisoprolol 5 mg prior to each cycle and didn’t develop any arrhythmia in subsequent cycles.
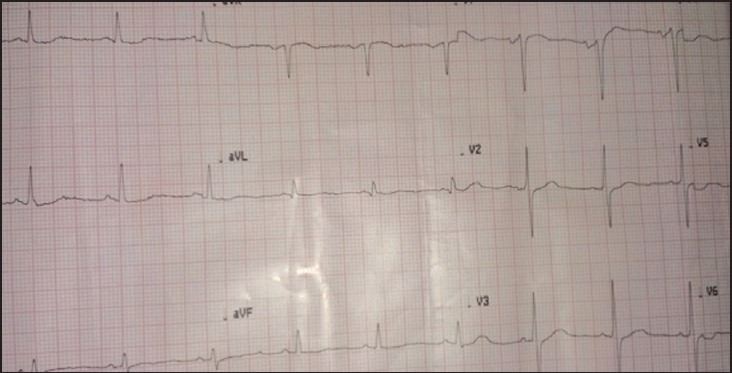
| Fig. 1a Serial electrocardiograms
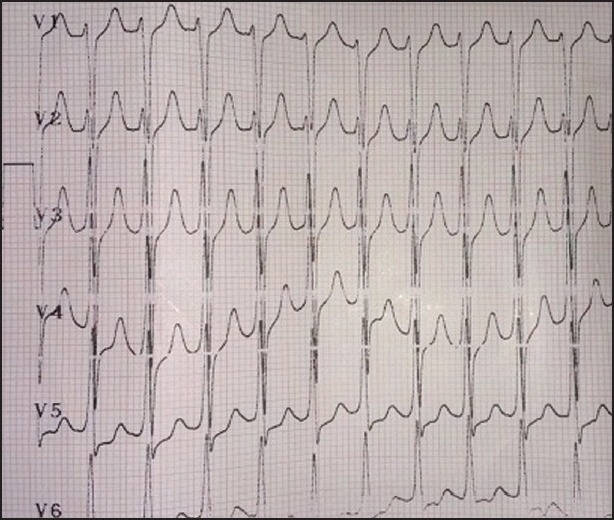
| Fig. 1b Serial electrocardiograms
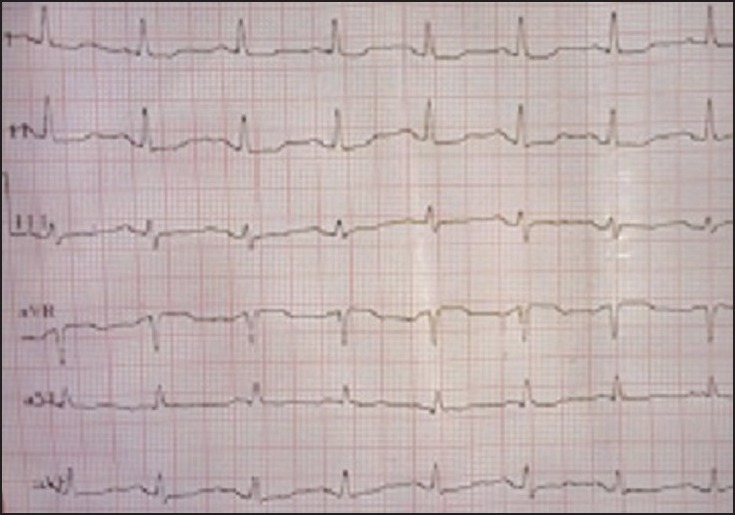
| Fig. 1c Serial electrocardiograms
DISCUSSION
Cisplatin is a potent chemotherapeutic drug that is used in a broad range of cancers.[1] It was first described by M. Peyrone in 1845 and was known for a long time as Peyrone's salt.[2] Cisplatin was approved for use in testicular and ovarian cancers by the U.S. Food and Drug Administration on December 19, 1978. The use of Cisplatin is limited by its toxicity that includes nephrotoxicity, neurotoxicity, gastrointestinal side effects, ototoxicity and others. Cardiotoxicity due to cisplatin includes electrocardiographic changes, arrhythmias, myocarditis, cardiomyopathy and congestive heart failure. Entire spectrum of arrhythmia, including supraventricular tachycardia, bradycardia and block in any degree may be observed during or shortly after cisplatin administration, some of them being clinically important and may cause death.[3] Cardiac toxicity of Cisplatin can be either due to a direct toxic action on cardiac myocytes or due to reactive oxygen species (ROS) production and the subsequent induction of oxidative stress and switch to a prothrombotic condition.[4,5] However, it is known that cisplatin frequently induces alterations in the electrolyte balance, in particular intracellular and extracellular potassium and magnesium concentrations. Such electrolyte imbalances are likely to play a significant role in the pathogenesis of cisplatin-induced arrhythmias.[6] Ozlem et al. studied the prevalence of silent arrhythmia in patients receiving cisplatin-based chemotherapy. They found cisplatin-related acute arrhythmia in any degree in as many as 66.7%, all which were silent. They concluded that the mechanism of cisplatin induced cardiac arrhythmias seems to be independent of changes in the serum electrolyte levels and may be due to the direct effect of the drug on cardiac sodium channels leading to an increase in QT dispersion or any other mechanism, which may cause inhomogeneity of ventricular recovery.[7] In addition to arrhythmias, cisplatin also produces cardiac dysfunction predominantly diastolic, whereas the rate of systolic dysfunction remains low. Several agents have been investigated for the potential role in ameliorating the cardiotoxicity of cisplatin.[8,9] Resveratrol, acetyl-l-carnitine, DL-α-lipoic acid and silymarin have been found to protect cardiomyocytes from cisplatin-induced cardiotoxicity.
Our patient didn’t have a history of any cardiac ailment and developed PSVT during cisplatin infusion that reverted back once cisplatin infusion was stopped. Electrolytes were normal. His cardiac evaluation including echocardiography and electrophysiological studies were normal. Thus, it was concluded that PSVT in this patient was secondary to cisplatin induced cardiotoxicity. Patient received subsequent cycles of chemotherapy without any problems.
CONCLUSION
Cisplatin is a useful antineoplastic drug with activity against a broad range of cancers. However, toxicity due to cisplatin is quite common and may result in stoppage of the drug. Cardiotoxicity of cisplatin can be symptomatic or symptomatic. Several antioxidants are being evaluated for a protective role in preventing cisplatin induced cardio toxicity.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
| Fig. 1a Serial electrocardiograms
| Fig. 1b Serial electrocardiograms
| Fig. 1c Serial electrocardiograms