 PDF
PDF  Views
Views  Share
Share


Clinical, Morphological, and Molecular Study of Diffuse WHO Grade II and III Astrocytomas: A Retrospective Analysis from a Single Tertiary Care Institute
CC BY-NC-ND 4.0 ? Indian J Med Paediatr Oncol 2021; 42(06): 569-576
DOI: DOI: 10.1055/s-0041-1741061
Abstract
Introduction?Astrocytomas are the most common gliomas, classified on the basis of grade and?IDH?mutation status according to the World Health Organization (WHO) 2016 update.?IDH?mutations are seen in 70 to 80% of diffuse grade II and III astrocytomas and are associated with better outcome. They serve as predictive biomarker in?IDH-targeted therapies such as small-molecule inhibitors or vaccines.
Objective?The aim of this study was to analyze the clinical, morphological, immunohistochemical, and molecular genetic characteristics of diffuse astrocytoma (DA: grades II and III). The?IDH?mutant and wild-type tumors are compared and contrasted with survival analysis on follow-up.
Materials and Methods?This was a retrospective study conducted on surgically resected tumor specimens. The hematoxylin and eosin-stained slides were examined for histologic features. Immunohistochemistry (IHC) was performed using?IDH1R132H,?ATRX, p53, and?Ki67. All cases of negative immunohistochemical expression of?IDH1R132H?were subjected to?IDH1?mutation analysis by Sanger sequencing. Overall survival was estimated by the Kaplan-Meier method using the log-rank (Mantel?Cox) test.
Results?The study included 51 cases of DA in the age of 17 to 66 years, mean???standard deviation was 35.5???9.7 years, and male:female ratio was 2:1.The?IDH1R132H?cytoplasmic immunopositivity was seen in 36 cases (70.5%), of which 63.6% were of grade II and 72.5% were of grade III.?ATRX?showed loss of expression in 50 cases (98%), and?p53?showed diffuse strong immunohistochemical expression in all the cases of?IDH?mutant tumors. The difference in the age at presentation for?IDH?mutant (32.5 years) and wild type tumors (38 years) was statistically significant. Median survival was 55.3 months and 22.2 months in of?IDH?mutant and wild type cases, respectively.
Conclusion?IHC and sequencing for IDH mutations is helpful in making an integrated diagnosis and classifying definite molecular subgroups of astrocytic tumors. Mutations in IDH core-elate with survival. IDH mutant tumors showed longer survival duration and are good prognostic indicators.
Keywords
glioma - diffuse astrocytoma - immunohistochemistry -?IDH1/2?mutations - Sanger sequencing - survivalPublication History
31 December 2021 (online)
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Abstract
Introduction?Astrocytomas are the most common gliomas, classified on the basis of grade and?IDH?mutation status according to the World Health Organization (WHO) 2016 update.?IDH?mutations are seen in 70 to 80% of diffuse grade II and III astrocytomas and are associated with better outcome. They serve as predictive biomarker in?IDH-targeted therapies such as small-molecule inhibitors or vaccines.
Objective?The aim of this study was to analyze the clinical, morphological, immunohistochemical, and molecular genetic characteristics of diffuse astrocytoma (DA: grades II and III). The?IDH?mutant and wild-type tumors are compared and contrasted with survival analysis on follow-up.
Materials and Methods?This was a retrospective study conducted on surgically resected tumor specimens. The hematoxylin and eosin-stained slides were examined for histologic features. Immunohistochemistry (IHC) was performed using?IDH1R132H,?ATRX, p53, and?Ki67. All cases of negative immunohistochemical expression of?IDH1R132H?were subjected to?IDH1?mutation analysis by Sanger sequencing. Overall survival was estimated by the Kaplan-Meier method using the log-rank (Mantel?Cox) test.
Results?The study included 51 cases of DA in the age of 17 to 66 years, mean???standard deviation was 35.5???9.7 years, and male:female ratio was 2:1.The?IDH1R132H?cytoplasmic immunopositivity was seen in 36 cases (70.5%), of which 63.6% were of grade II and 72.5% were of grade III.?ATRX?showed loss of expression in 50 cases (98%), and?p53?showed diffuse strong immunohistochemical expression in all the cases of?IDH?mutant tumors. The difference in the age at presentation for?IDH?mutant (32.5 years) and wild type tumors (38 years) was statistically significant. Median survival was 55.3 months and 22.2 months in of?IDH?mutant and wild type cases, respectively.
Conclusion?IHC and sequencing for IDH mutations is helpful in making an integrated diagnosis and classifying definite molecular subgroups of astrocytic tumors. Mutations in IDH core-elate with survival. IDH mutant tumors showed longer survival duration and are good prognostic indicators.
Keywords
glioma - diffuse astrocytoma - immunohistochemistry -?IDH1/2?mutations - Sanger sequencing - survival
Introduction
The World Health Organization (WHO) 2016 update brought in paradigm changes in understanding and classification of central nervous system neoplasms bringing in the molecular biology of these tumors.[1] The adult diffuse gliomas are essentially classified on the basis of?IDH?mutations, which have been observed to be an important prognostic and predictive biomarker.[1] [2] [3]?IDH?mutations are reported in >80% of WHO grade II/III gliomas.[4] Other studies have reported?IDH?mutations in 72% of grade II and 64% of grade III astrocytomas.[5] [6] Diffuse gliomas that do not harbor?IDH?mutations exhibit aggressive behavior irrespective of the grade of the tumor.?IDH?wild-type diffuse astrocytoma (DA) and anaplastic astrocytoma (AA) have a survival similar to or only slightly longer than?IDH?wild-type glioblastoma.[2] [3] [4] [7] [8] Presence of?EGFR?amplification and a genotype of?7q?gain and?10q?loss have been associated with worse outcome.[9] Study of?IDH?mutations alone in diffuse glioma is an important research tool for targeted therapies and possible vaccines.
In this article, we share our experience with diffuse astrocytic tumors, WHO grades II and III, with respect to clinical features, histopathology, and molecular studies. The survival was compared between two molecular subgroups.
Materials and Methods
Study Design: This was a retrospective evaluation of the clinical, histopathological, and molecular markers of WHO grade II and III astrocytomas. The?IDH?mutant and wild-type tumors have been compared with respect to survival.
Study Setting: The study was performed in a tertiary care center. The study period was from January 2015 to June 2017.
Participants:?All patients diagnosed on histopathology as grade II or III astrocytoma were included in all age groups. Other types of gliomas were excluded.
Variables: The astrocytomas were classified into?IDH?mutant and wild-type gliomas. The two molecular types were compared with respect to demographic features, location, survival, and outcome.
Primary Outcome: Comparison of the longest survival period between?IDH?mutant and wild-type tumors.
Secondary Outcome: Comparison of other variables like age, location, and histopathology between?IDH?mutant and wild-type tumors.
Data Collection: The patient details including demographic features, clinical presentation, and radio imaging findings were obtained from the request forms. The treatment details were obtained from medical records. The duration of the follow-up was calculated on the basis of last follow-up date or death of the patient, whichever was earlier.
Histopathology
The tumor specimens were fixed in formalin and processed routinely. The hematoxylin and eosin-stained slides were examined for histologic features of DA and categorized into grade II or III as per the WHO 2016 Classification.[1]
Immunohistochemistry (IHC)
This was performed using?IDH1R132H?(clone D09, Dianova, dilution 1:200),?ATRX?(HPA001906, Sigma Aldrich, dilution 1:500),?p53?(Clone D07, Bio-Genex), and?Ki67?(Sigma Aldrich, Ready to Use). Cytoplasmic staining for?IDH1R132H?and nuclear staining for?ATRX,?p53, and?Ki67?were interpreted as positive
Sequencing
All cases of negative?IDH1R132H?immunoexpression were subjected to?IDH?mutation analysis by Sanger sequencing.
DNA Extraction FFPE Tissue
Formalin-fixed, paraffin-embedded (FFPE) blocks were cut into 12 serial sections of 18??m each. Areas consisting of at least 80% tumor cells were marked on the unstained sections that were then scraped into polypropylene tubes and deparaffinized using xylene. The collected tumor tissue was subjected to deoxyribonucleic acid (DNA) extraction with the QIAmp DNA FFPE Tissue kit following manufacturer's protocol. Isolated DNA concentration was quantified by spectrophotometry using Nano drop 2000 instrument.
IDH?Mutation Analysis
Polymerase chain reaction (PCR) amplification of the target region was performed by mixing 50?ng of extracted tumor DNA as template, 10 ?L of HotStar Taq 2X Mastermix (DSS Takara), 200?nM of the respective forward and reverse primers, and high-purity water to a final volume of 20 ?L (IDH1?PCR primers: forward, AATGAGCTCTATATGCCATCACTG; reverse, TTCATACCTTGCTTAATGGGTGT). The PCR cycling conditions included an initial denaturation step at 95?C for 5?minutes, followed by 40 cycles of denaturation at 95?C for 30?seconds, annealing at 60?C for 30?seconds, and elongation at 72?C for 30?seconds, concluding with a final elongation step at 72?C for 10?minutes. The PCR products were checked by electrophoresis on 2% agarose gel. Amplified PCR products were subjected to Sanger sequencing for detection of mutations in?IDH1?gene.
Fluorescence In Situ Hybridization
Fluorescence in situ hybridization (FISH) was performed on FFPE sections using dual color locus specific probes for?1p36?and?19q13?paired, respectively, with the reference probes for?1q25?and?19p13?(Vysis). This test was performed in the study group in?IDH?mutant gliomas if the?ATRX?immunoexpression was retained. Following pretreatment, probes were added to the sections and the slides were subjected to denaturation at 78?C for 5?minutes and hybridization at 37?C for 16?hours in thermobrite chamber. After counter staining with 4?,6-diamidino-2-phenylindole, slides were examined under fluorescent microscope. The hybridization signals were scored in at least 200 nonoverlapping nuclei. The ratio of?1p/1q?and?19q/19p?was calculated by taking the number of test and control signals. Also, 1:2 ratio of signals in >50?lls was taken as a criteria for codeletion.[10]
Sample Size:?The study included 51 patients. All consecutive cases diagnosed as DA WHO grades II and III were included in the study period.
Statistical Analysis
Demographic and other relevant clinical data were presented as mean or proportioned appropriately. Statistical analysis was performed using Graph Pad Prism 8.4.3. Data were analyzed and correlation was done between?IDH?mutation status and grading of astrocytoma. Overall survival (OS) was defined as the interval between primary surgery and death or last follow-up. OS was estimated by the Kaplan-Meier method using the log-rank (Mantel?Cox) test. A?p-value less than 0.05 was considered to be of statistical significance.
Interpretation of Testing ([Table 1])
|
IDH mutant astrocytoma, WHO grade II (N?=?7) |
IDH wild type astrocytoma, WHO grade II (N?=?4) |
IDH mutant astrocytoma, WHO grade III (N?=?31) |
IDH wild type astrocytoma, WHO grade III (N?=?9) |
|
|---|---|---|---|---|
|
Age group (years) |
17?40 |
29?45 |
18?66 |
25?55 |
|
Male:female ratio |
0.75:1 |
3:1 |
3.8:1 |
0.9:1 |
|
Common location |
Frontal and temporal lobes |
Temporal |
Frontal |
Frontal |
|
Mean age |
29 years |
38 years |
36 years |
38 years |
|
Overall survival (months) |
63 |
N/A |
60 |
90 |
|
Median survival (months) |
60 |
N/A |
56 |
38 |
.jpg)
|?Graph 1 Age distribution among grade II and III astrocytomas.
Most common clinical presentation of the patients was headache (33, 70%) followed by seizures (25, 53%) and weakness of limbs, and the most common location of tumor was frontal lobe (14, 32%).
The magnetic resonance imaging findings were reviewed and correlated with final histopathology. Thirteen cases of grade III astrocytoma were considered to be low-grade glioma due to absence of perilesional edema and contrast enhancement, whereas three cases of grade II astrocytoma were considered to be of high grade due to extensive perilesional edema and mass effect. Apart from these, there was correlation of radio imaging and histopathological features. Two cases, one each of grades II and III, had pattern of gliomatosis cerebri.
The surgical notes mentioned that 62% of the tumors had gross total resection.
Histomorphology
WHO grade II astrocytoma constituted 11/51 (21.6%) cases. These tumors showed increased cellularity and pleomorphism without atypical mitosis. WHO grade III astrocytoma constituted 40/51 (78.4%) cases. These tumors showed hypercellularity, pleomorphism, and atypical mitosis. Atypical mitosis was more than one per section in grade III tumors. Microcystic spaces were identified in 11/51 (21.5%) tumors. Focal oligodendroglial pattern was observed in 2/51 (3.9%) grade III tumors and these resembled the erstwhile oligoastrcotyomas. Tumor calcification was identified in only one (1.9%) grade III tumor. Gemistocytes were observed in 15/51 (29.4%) cases, of which 13 belonged to grade III. Necrosis and microvascular proliferation, which are typical features of grade IV tumors, were absent in all cases.
Immunohistochemistry
IDHR132H:?The cytoplasmic immunopositivity was seen in 36/51 (70.5%) cases, of which 63.6% were grade II and 72.5% were grade III.
ATRX:?The?ATRX?showed loss of expression in 50 cases whereas one?IDH?mutant AA (grade III) showed retained?ATRX?nuclear expression, but this case did not show?1p19q?codeletion on FISH analysis. Of the cases that were negative for?IDH1R132H, five had loss of?ATRX?expression.
p53:?There was diffuse strong immunohistochemical expression of?p53?in all the cases of?IDH?mutant tumors. Among 15 tumors that were negative for?IDH1R132H, 6 showed diffuse?p53?expression whereas the rest 9 were negative.
Ki67:?The mean???SD?Ki67?for grade II tumors was 2.36???1.0 (range: 1?5) and grade III tumors was 15.6???11.3 (range: 6?64).
Sequencing
Out of the 15 tumors that were negative for?IDH1R132H?IHC, only 2 cases (both belonging to grade III) showed mutations in Sanger sequencing as depicted in [Fig. 1]. These mutations were also identified in?IDH1R132H?locus. None of the cases showed any other?IDH1?mutations.
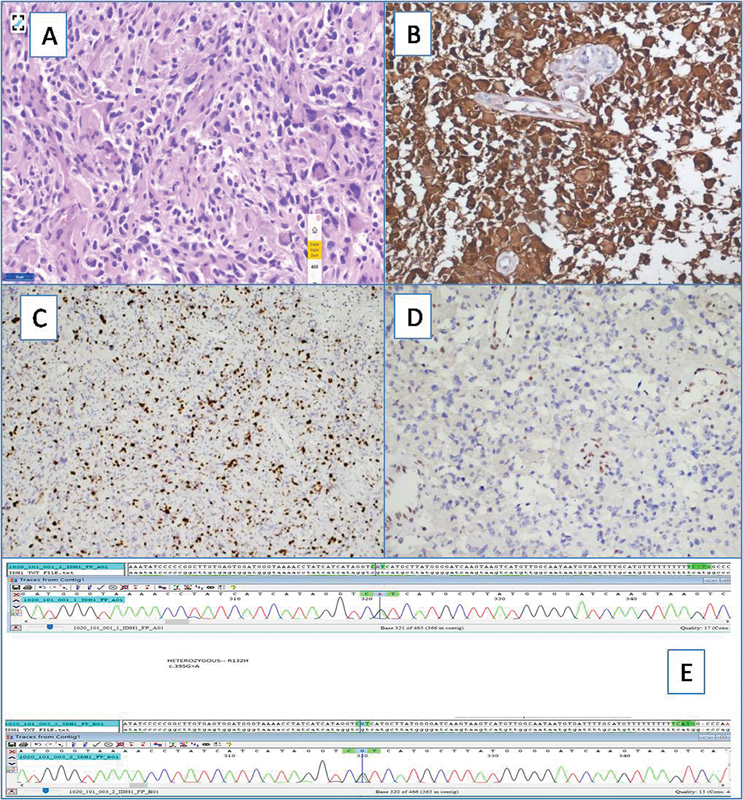
|?Fig. 1 (Top) Microscopic images of a grade III anaplastic astrocytoma. (A) Cellular tumor with marked pleomorphism and atypia showing many gemistocytes (H&E ?40). (B) Cytoplasmic positivity for IDH1R132H; HRP-polymer ?100. (C) Tumor cells showing diffuse strong expression of p53; HRP-polymer ?40. (D) Loss of ATRX expression; HRP-polymer ?100. (E) IDH1 polymerase chain reaction products (500?bp length) run on 2% agarose gel; ethidium bromide used as deoxyribonucleic acid (DNA) staining dye. (Bottom) Detection of DNA changes at R132 locus (R132H mutation, G?>?A) in two cases of IDH1R132H immunohistochemistry negative astrocytoma.
Applying integrated diagnosis, 74.5% tumors in this study were?IDH?mutant.
Follow-Up Period and Survival
Follow-up data were available in 37/51 patients. All these patients were given 54 Gy of intensity modulated radiotherapy (IMRT) and chemotherapy with temozolomide for a period ranging from 31 to 1,488 days and a mean of 374???269.4 days. All the patients were followed up for a period of 2 days to 90 months. The follow-up and survival analysis were done separately for?IDH?mutant and?IDH?wild-type astrocytomas. The OS was 48.6%, and 51.4% patients died at the end of follow-up period. Eighteen of the patients are alive at the longest follow-up including 14?IDH?mutant and 4?IDH?wild-type patients. The OS differed in grades with 57.2% in grade II and 46.7% in grade III astrocytomas.
Recurrence of tumors occurred in 11 (29.7%) cases at the mean???SD interval of 85???68.4 days. In two of these patients, the tumors upgraded from grade II to grade III.
The?IDH?mutant and wild-type patients were compared for
age, M:F ratio, location, and median survival by calculating?p-value using
chi-square test. The?p-value was statistically significant (p?
<!--?0.001) for the age distribution showing difference in age at diagnosis between?
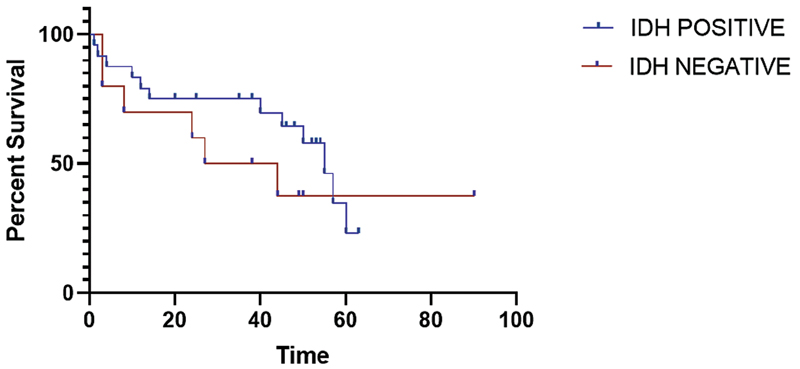
The patient survival period was calculated by Kaplan-Meier survival analysis. Median survival was 55.3
months and 22.2 months in?IDH?mutant and?IDH?wild-type cases, respectively. From the survival analysis, it was evident that
patients with?IDH?mutations had better survival. Log-rank
(Mantel?Cox) test was done for comparison of survival curves, which did not show any significance between these
groups. This is shown in [Graphs 2] and [3].
|?Graph 2 Kaplan-Meier survival analysis of IDH mutant grade
II and III and IDH wild type grade III astrocytomas.
|?Graph 3Kaplan-Meier survival analysis of IDH mutant and IDH
wild type astrocytomas. The survival analysis showed that?IDH?wild-type grade III tumors had least median survival period with poor prognosis.
DA is a common brain tumor mainly affecting young adults, and encompasses ?11 to 15% of all astrocytic
brain tumors. In older adults over 40, the age-adjusted annual incidence rate of astrocytic tumors is 6.8/100,000
people.[6] [11] [12] DA and AA are defined as tumors that lack the?1p/19q?codeletion and usually demonstrate loss of
expression of?ATRX?and express mutant?p53?protein. IDH?mutant and wild-type astrocytomas are clinically
different tumors despite overlapping histological appearances.?IDH?mutations are the driving mutations in gliomagenesis, identified in 70 to 80% of
DA. Majority of these mutations are?IDH1?type, commonest
being?IDH1R132H.[13] IHC for?IDH1R132H?is a surrogate for the
mutation, and DNA sequencing is advocated only for the rare?IDH1/2?mutations whenever diffuse gliomas are immunonegative for?IDH1R132H.[6] In this study, DA constituted 21.7% (51/234) of all the primary brain tumors in the study period. This
is comparable to the study by Watanabe et al[6] (29.5%), however is lesser than that reported by Rajeswarie et al[14] (47.5%). The distribution of grades is similar to these two studies. The mean age at presentation in our patients was 35.5???9.7 years, which is comparable to that reported
in other studies.[11] [12] [14]?IDH?mutant gliomas have been found to have
earliest age at diagnosis. The most common presenting complaint was headache (70%) followed by seizures (53%), which is comparable
to the study by Mu et al.[11] Most common location in this study was frontal lobe (32%) consistent with findings by
Rajeswarie et al[14] (41% in grade II and 46.4% in grade III), Dong et al,[15] and Mu et al.[11] IHC with?IDH1R132H?was positive in 70.5?ses, of which
19.4?longed to grade II and 80.5?longed to grade III. Study by Mu et al[11] observed?IDH1R132H?positivity in 77% of DA
(19% of grade II and 81% of grade III). Median age of?IDH1R132H?mutant astrocytoma was 32 years, which is comparable to other studies. ATRX?mutations have been reported either by sequencing or IHC
in 45 to 67% of DA and 57 to 73% of AA.[16] [17] [18] [19] The mutations in?ATRX?are supposed to
follow?IDH?mutations for astrocytic phenotype in a diffuse glioma.
These are mutually exclusive of?1p19q?codeletion. A surrogate IHC
with loss of nuclear staining for?ATRX?in neoplastic cells, with
retention in nonneoplastic cells serving as an internal positive control, is a reliable indicator of?ATRX?mutations.[20] Inactivation of the adenosine triphosphate-dependent helicase?ATRX?has been linked to recombination-driven alternative telomere maintenance
mechanisms and may provide glioma cells with unlimited proliferative capacity.[21] [22] [23] In this study, 97.5% of?IDH?mutant
astrocytoma showed loss of?ATRX. The WHO 2016 eliminated oligoastrocytoma as a distinct entity, since nearly all histologically defined
oligoastrocytoma can be recategorized as oligodendroglioma or astrocytoma based on molecular features.[24] We observed two cases of oligoastrocytoma that could be reliably classified as?IDH?mutant astrocytoma due to loss of?ATRX?and diffuse?p53?positivity.
Another case of?IDH?mutant grade III astrocytoma with
retained?ATRX?did not show?1p19q?co deletion hence was classified as astrocytoma. Tumorigenic?Tp53?mutations have been reported to be
present in >50% of gliomas with astrocytic features, including 59 to 74% of DA and 53 to 65% of AA.[4] In this study, diffuse and strong positivity for?p53?was observed in all cases of?IDH?mutant astrocytoma. Grade II and III astrocytomas, which showed diffuse and strong
positivity for?p53, constituted 72.8 and 91.6%, respectively. Pediatric DA is distinct clinically and molecularly from their adult counterparts. Clinical
implications of?BRAF?alterations in these tumors and behavior of
tumors with?MYB/MYBL1/FGFR?alterations are less clear.[25] Although extremely common in adult diffuse glioma,?IDH1/2?mutations are much less prevalent in pediatric gliomas. Previous reports
suggested extremely low numbers of?IDH?mutants in pediatric gliomas
ranging from 0 to 17%.[25] In this study we noticed two pediatric patients with diffuse?IDH?mutant astrocytoma accounting for 2/40 (5%) of cases. These tumors are known to
behave like adult?IDH?mutant astrocytoma. We did not identify any
case of?IDH?wild type pediatric DA in our series. Loss of the?CDKN2A?gene or?p16?protein (the?CDKN2A?product)
appears an ideal candidate for distinguishing the molecular phenotypes of WHO grade II and III?IDH?mutant gliomas. Studies showed that?CDKN2A?loss is associated with worse survival in astrocytoma.[26] Available evidence from retrospective studies suggests that homozygous deletion
of?CDKN2A/B?is associated with shorter survival in patients
with?IDH?mutant astrocytoma and that its presence corresponds to WHO
grade IV clinical behavior.[27] [28] However, the molecular study was limited to identification of?IDH?mutation status, and other mutations that cause astrocytoma were not identified in
this study. Survival patterns for lower-grade astrocytoma remain poorly characterized. Several independent projects
have demonstrated that histologic grading standards probably cannot distinguish prognoses for patients
with?IDH?mutant astrocytoma in the WHO grade II and III entities.[29] [30] On the contrary, some studies have concluded that traditional grading system is still able
to stratify prognoses for these patients.[31] [32] [33] In this study, all grade II and III DA patients with available follow-up received combined 54 Gy of
IMRT and chemotherapy with temozolomide for a period ranging from 31 to 1,488 days and a mean of 374 days, while the
study by Mu e tal[11] observed that 48.6% received both chemotherapy and radiotherapy and 51.4% received only
radiotherapy. Study by Dong et al[15] observed 52.69% of grade II and 77.35% of grade III tumors receiving radiation. The prognostic importance of?IDH?mutation is independent
of other known prognostic factors, including age, grade, and?MGMT?methylation status.[34]?IDH?mutations exhibit?G-CIMP?signature in glioma and the gliomagenesis has been attributed to the
oncometabolite, 2-hydroxyglutarate (2-HG). This results in DNA and histone methylation. 2-HG is a part of DNA repair
pathway and serves as an inhibitor of DNA repair enzymes as well as inhibits the homologous recombination DNA repair
process. This helps in targeting the DNA repair enzymes by chemoradiotherapy giving a therapeutic
benefit.?IDH?mutant tumors are also common in surgically amenable
sites and gross total resection gives additional survival advantage. The second mutant protein,?ATRX, is a chromatin-binding protein (SNF?family)
and the mutations result in telomere dysfunction.?ATRX?deficiency is
associated with genomic instability that can induce?p53-dependent cell
death. So?p53?mutations in DA may enable tumor cell survival in the
setting of?ATRX?loss.[35] Studies showed that median survival of grade II and grade III astrocytomas is 7 to 10 years and 3.5
years, respectively.[33] Pekmezci et al[32] observed median OS is better in patients with?IDH?mutant astrocytoma (9.3 years) than?IDH?wild-type astrocytoma (1.2 years). Another study identified that the median
survival of?IDH?wild-type gliomas was 1.7 years as against 6.3 years
for?IDH?mutant gliomas without?1p19q?codeletion.[3] The similar was observed in our study with a median survival of 55.3 months (4.6 years) and
22.2 months (1.9 years) in?IDH?mutant and wild-type astrocytomas,
respectively. However, this difference was not found to be statistically significant. This could perhaps be related
to less number of?IDH?wild-type cases. In a study by Shirahata et al,[33] it was identified that there was difference in survival of?IDH?mutant tumors. On follow-up, survival of 31.7% of?IDH?mutant glioblastomas and 42.6% of?IDH?mutant AA was similar and this was associated with?CDKN2A/B?homozygous deletion. However, we did a similar comparison of median survival
of?IDH?mutant AA with?IDH?mutant glioblastomas in the same period. We identified 61.7% of?IDH?mutant AA with median survival of 55.3 months and 7.3% of?IDH?mutant glioblastomas with median survival of 12 to 15 months. However,
we need to confirm these findings further by performing?CDKN2A/B?deletion studies and expanding the sample size. Limitations:?The limitations of this study are retrospective
study design. The follow-up details of all the patients were not available. Limited sample size of 51 patients is
also a limitation for a complete statistical analysis. Future Research Directions:?There are advances in molecular
genetics of diffuse gliomas including astrocytoma. The?IDH?mutant
tumors are further classified based on?CDKN2A/B?homozygous deletions.
The tumors with these deletions are shown to have aggressive behavior even in?IDH?mutant tumors. We plan to perform this deletion analysis and correlate with
patient survival. In conclusion, we observed that IHC with?IDH1R132H,?ATRX, and?p53?is helpful in making an integrated diagnosis of astrocytic tumors as per the
updated 2016 WHO classification of tumors. Other studies have also shown utility of IHC in subtyping the gliomas and
our results are similar to these studies. Classification into definite molecular subgroups by sequencing to find out
other variant?IDH1?or?IDH2?mutations is necessary according to WHO guidelines.?IDH?mutations correlate with survival and are good prognostic indicators in DA. Nil.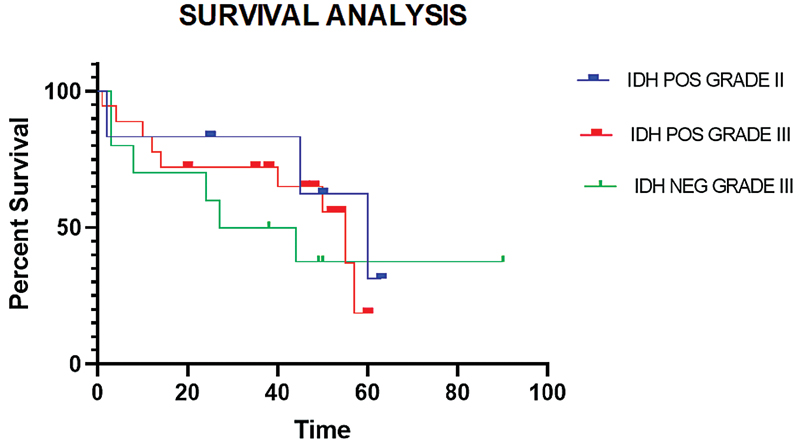
Discussion
Conclusion
Conflict of Interest
References
Address for correspondence
Publication History
31 December 2021 (online)
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
|?Graph 1Age distribution among grade II and III astrocytomas..
|?Fig. 1 (Top) Microscopic images of a grade III anaplastic astrocytoma. (A) Cellular tumor with marked pleomorphism and atypia showing many gemistocytes (H&E ?40). (B) Cytoplasmic positivity for IDH1R132H; HRP-polymer ?100. (C) Tumor cells showing diffuse strong expression of p53; HRP-polymer ?40. (D) Loss of ATRX expression; HRP-polymer ?100. (E) IDH1 polymerase chain reaction products (500?bp length) run on 2% agarose gel; ethidium bromide used as deoxyribonucleic acid (DNA) staining dye. (Bottom) Detection of DNA changes at R132 locus (R132H mutation, G?>?A) in two cases of IDH1R132H immunohistochemistry negative astrocytoma.
|?Graph 2 Kaplan-Meier survival analysis of IDH mutant grade II and III and IDH wild type grade III astrocytomas.
|?Graph 3Kaplan-Meier survival analysis of IDH mutant and IDH wild type astrocytomas.
References
- ry A, Reifenberger G. et al.?The 2016 World Health Organization Classification of Tumors of the Central Nervous System: a summary. Acta Neuropathol 2016; 131 (06) 803-820
- rat DJ, Verhaak RG, Aldape KD. et al; Cancer Genome Atlas Research Network.?Comprehensive, integrative genomic analysis of diffuse lower-grade gliomas. N Engl J Med 2015; 372 (26) 2481-2498
- ckel-Passow JE, Lachance DH, Molinaro AM. et al.?Glioma groups based on 1p/19q, IDH, and TERT promoter mutations in tumors. N Engl J Med 2015; 372 (26) 2499-2508
- an H, Parsons DW, Jin G. et al.?IDH1 and IDH2 mutations in gliomas. N Engl J Med 2009; 360 (08) 765-773
- artmann C, Meyer J, Balss J. et al.?Type and frequency of IDH1 and IDH2 mutations are related to astrocytic and oligodendroglial differentiation and age: a study of 1,010 diffuse gliomas. Acta Neuropathol 2009; 118 (04) 469-474
- atanabe T, Nobusawa S, Kleihues P, Ohgaki H.?IDH1 mutations are early events in the development of astrocytomas and oligodendrogliomas. Am J Pathol 2009; 174 (04) 1149-1153
- artmann C, Hentschel B, Wick W. et al.?Patients with IDH1 wild type anaplastic astrocytomas exhibit worse prognosis than IDH1-mutated glioblastomas, and IDH1 mutation status accounts for the unfavorable prognostic effect of higher age: implications for classification of gliomas. Acta Neuropathol 2010; 120 (06) 707-718
- eller M, Weber RG, Willscher E. et al.?Molecular classification of diffuse cerebral WHO grade II/III gliomas using genome- and transcriptome-wide profiling improves stratification of prognostically distinct patient groups. Acta Neuropathol 2015; 129 (05) 679-693
- rat DJ, Aldape K, Colman H. et al.?cIMPACT-NOW update 3: recommended diagnostic criteria for ?Diffuse astrocytic glioma, IDH-wildtype, with molecular features of glioblastoma, WHO grade IV?. Acta Neuropathol 2018; 136 (05) 805-810
- Suri V, Jha P, Agarwal S. et al.?Molecular profile of oligodendrogliomas in young patients. Neuro-oncol 2011; 13 (10) 1099-1106
- Mu L, Xu W, Li Q. et al.?IDH1 R132H mutation is accompanied with malignant progression of paired primary-recurrent astrocytic tumours. J Cancer 2017; 8 (14) 2704-2712
- Cohen AL, Holmen SL, Colman H.?IDH1 and IDH2 mutations in gliomas. Curr Neurol Neurosci Rep 2013; 13 (05) 345
- Santosh V, Sravya P, Gupta T. et al.?ISNO consensus guidelines for practical adaptation of the WHO 2016 classification of adult diffuse gliomas. Neurol India 2019; 67 (01) 173-182
- Rajeswarie RT, Rao S, Nandeesh BN, Yasha TC, Santosh V.?A simple algorithmic approach using histology and immunohistochemistry for the current classification of adult diffuse glioma in a resource-limited set-up. J Clin Pathol 2018; 71 (04) 323-329
- Dong X, Noorbakhsh A, Hirshman BR. et al.?Survival trends of grade I, II, and III astrocytoma patients and associated clinical practice patterns between 1999 and 2010: a SEER-based analysis. Neurooncol Pract 2016; 3 (01) 29-38
- Christians A, Adel-Horowski A, Banan R. et al.?The prognostic role of IDH mutations in homogeneously treated patients with anaplastic astrocytomas and glioblastomas. Acta Neuropathol Commun 2019; 7 (01) 156
- Jiao Y, Killela PJ, Reitman ZJ. et al.?Frequent ATRX, CIC, FUBP1 and IDH1 mutations refine the classification of malignant gliomas. Oncotarget 2012; 3 (07) 709-722
- Liu XY, Gerges N, Korshunov A. et al.?Frequent ATRX mutations and loss of expression in adult diffuse astrocytic tumors carrying IDH1/IDH2 and TP53 mutations. Acta Neuropathol 2012; 124 (05) 615-625
- Wiestler B, Capper D, Holland-Letz T. et al.?ATRX loss refines the classification of anaplastic gliomas and identifies a subgroup of IDH mutant astrocytic tumors with better prognosis. Acta Neuropathol 2013; 126 (03) 443-451
- Ebrahimi A, Skardelly M, Bonzheim I. et al.?ATRX immunostaining predicts IDH and H3F3A status in gliomas. Acta Neuropathol Commun 2016; 4 (01) 60
- Barthel FP, Wei W, Tang M. et al.?Systematic analysis of telomere length and somatic alterations in 31 cancer types. Nat Genet 2017; 49 (03) 349-357
- Clynes D, Jelinska C, Xella B. et al.?Suppression of the alternative lengthening of telomere pathway by the chromatin remodelling factor ATRX. Nat Commun 2015; 6: 7538
- Heaphy CM, de Wilde RF, Jiao Y. et al.?Altered telomeres in tumors with ATRX and DAXX mutations. Science 2011; 333 (6041): 425
- Sahm F, Reuss D, Koelsche C. et al.?Farewell to oligoastrocytoma: in situ molecular genetics favor classification as either oligodendroglioma or astrocytoma. Acta Neuropathol 2014; 128 (04) 551-559
- Pollack IF, Hamilton RL, Sobol RW. et al; Children's Oncology Group.?IDH1 mutations are common in malignant gliomas arising in adolescents: a report from the Children's Oncology Group. Childs Nerv Syst 2011; 27 (01) 87-94
- Reis GF, Pekmezci M, Hansen HM. et al.?CDKN2A loss is associated with shortened overall survival in lower-grade (World Health Organization Grades II-III) astrocytomas. J Neuropathol Exp Neurol 2015; 74 (05) 442-452
- Brat DJ, Aldape K, Colman H. et al.?cIMPACT-NOW update 5: recommended grading criteria and terminologies for IDH-mutant astrocytomas. Acta Neuropathol 2020; 139 (03) 603-608
- Aoki K, Nakamura H, Suzuki H. et al.?Prognostic relevance of genetic alterations in diffuse lower-grade gliomas. Neuro-oncol 2018; 20 (01) 66-77
- Yoda RA, Marxen T, Longo L. et al.?Mitotic Index Thresholds do not predict clinical outcome for IDH-mutant astrocytoma. J Neuropathol Exp Neurol 2019; 78 (11) 1002-1010
- Cimino PJ, Zager M, McFerrin L. et al.?Multidimensional scaling of diffuse gliomas: application to the 2016 World Health Organization classification system with prognostically relevant molecular subtype discovery. Acta Neuropathol Commun 2017; 5 (01) 39
- Hasselblatt M, Jaber M, Reuss D. et al.?Diffuse astrocytoma, IDH-wildtype: a dissolving diagnosis. J Neuropathol Exp Neurol 2018; 77 (06) 422-425
- Pekmezci M, Rice T, Molinaro AM. et al.?Adult infiltrating gliomas with WHO 2016 integrated diagnosis: additional prognostic roles of ATRX and TERT. Acta Neuropathol 2017; 133 (06) 1001-1016
- Shirahata M, Ono T, Stichel D. et al.?Novel, improved grading system(s) for IDH-mutant astrocytic gliomas. Acta Neuropathol 2018; 136 (01) 153-166
- Sanson M, Marie Y, Paris S. et al.?Isocitrate dehydrogenase 1 codon 132 mutation is an important prognostic biomarker in gliomas. J Clin Oncol 2009; 27 (25) 4150-4154
- Han S, Liu Y, Cai SJ. et al.?IDH mutation in glioma: molecular mechanisms and potential therapeutic targets. Br J Cancer 2020; 122 (11) 1580-1589