 PDF
PDF  Views
Views  Share
Share


Clinicoepidemilogical Correlation of BRCA 1 and 2 Mutations in Carcinoma Ovary - an Indian Perspective
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2019; 40(04): 484-490
DOI: DOI: 10.4103/ijmpo.ijmpo_67_18
Abstract
Introduction: All over the world in 2008, approximately 225,000 women were diagnosed with ovarian cancer, and 140,000 died from this disease.[1] Ovarian cancer is the second-most common gynecologic malignancy in the developed countries. In the developing countries, it is the third-most common gynecologic malignancy after breast and cervical cancer with an incidence of 5.0/100,000 and a mortality rate of 3.1/100,000. Women with BRCA1 gene mutations typically develop ovarian cancer at an earlier age than other women, with an average age at diagnosis of 50-year-old while for patients with BRCA2 mutation carriers it is 60 years, similar to the general population. Aim and Objective: The aim of this study is to study the incidence, clinical profile, and outcomes of a patient with BRCA 1 and BRCA 2 mutation in carcinoma ovary and its comparison with patients without mutation. Results: Out of total 50 patients, 45 (90%) were BRCA negative and rest fi ve (10%) were BRCA positive. Of the five patients, only two (4% of total) had pathological mutations while the rest of three patients had benign mutations only. Overall median age of presentation was 61 years for BRCA-negative patients and 38 years for BRCA-positive patients. Most of the patients presented in Stage III (23 out of 50; 46%), while the second-most common presentation was in Stage IV (34%). In our study, we had an overall mortality of one patient who was BRCA negative, in Stage IV while no mortality was noted in BRCA positive subset of patients. Conclusion: This was a single center-based and spanned over 24 months involving limited number of patients with ovarian cancer with maximum follow-up for 9 months.
Publication History
Received: 25 March 2018
Accepted: 21 June 2018
Article published online:
03 June 2021
© 2020. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Abstract
Introduction: All over the world in 2008, approximately 225,000 women were diagnosed with ovarian cancer, and 140,000 died from this disease.[1] Ovarian cancer is the second-most common gynecologic malignancy in the developed countries. In the developing countries, it is the third-most common gynecologic malignancy after breast and cervical cancer with an incidence of 5.0/100,000 and a mortality rate of 3.1/100,000. Women with BRCA1 gene mutations typically develop ovarian cancer at an earlier age than other women, with an average age at diagnosis of 50-year-old while for patients with BRCA2 mutation carriers it is 60 years, similar to the general population. Aim and Objective: The aim of this study is to study the incidence, clinical profile, and outcomes of a patient with BRCA 1 and BRCA 2 mutation in carcinoma ovary and its comparison with patients without mutation. Results: Out of total 50 patients, 45 (90%) were BRCA negative and rest fi ve (10%) were BRCA positive. Of the five patients, only two (4% of total) had pathological mutations while the rest of three patients had benign mutations only. Overall median age of presentation was 61 years for BRCA-negative patients and 38 years for BRCA-positive patients. Most of the patients presented in Stage III (23 out of 50; 46%), while the second-most common presentation was in Stage IV (34%). In our study, we had an overall mortality of one patient who was BRCA negative, in Stage IV while no mortality was noted in BRCA positive subset of patients. Conclusion: This was a single center-based and spanned over 24 months involving limited number of patients with ovarian cancer with maximum follow-up for 9 months.
Keywords
BRCA 1 and 2 mutations - carcinoma ovary - germline mutationIntroduction
All over the world in 2008, approximately 225,000 women were diagnosed with ovarian cancer, and 140,000 died from this disease.[1] Ovarian cancer is the second-most common gynecologic malignancy in the developed countries, with an incidence of 9.4/100,000 women and a mortality rate of 5.1/100,000.
In the United States (US), there are approximately 22,000 new cases and 14,000 cancer-related deaths each year from this malignancy. It is the second-most common gynecologic malignancy in the US and the most common cause of gynecologic cancer death and the fifth leading cause of cancer death in women.[2] Based on data from the US National Cancer Database Surveillance, Epidemiology, and End Results, the annual incidence of ovarian cancer from 2005 to 2009 was 12.7/100,000 women.[3]
In the developing countries, it is the third-most common gynecologic malignancy after breast and cervical cancer with an incidence of 5.0/100,000 and a mortality rate of 3.1/100,000.
The majority of ovarian malignancies (95%) are derived from epithelial cells; the remainder arises from other ovarian cell types (germ cell tumors and sex cord-stromal tumors).[4] Serous carcinoma is regarded as closely related to fallopian tubal and peritoneal serous carcinoma, based on similarities in histology and clinical behavior.[5] Some experts have proposed that serous carcinomas all originate in the fallopian tubes. This is based on studies that detected fallopian tubal intraepithelial carcinoma in the fimbria of BRCA mutation carriers following risk-reducing bilateral salpingo-oophorectomy.
The lifetime risk of developing ovarian cancer in the US is 1.4%. The age at diagnosis of ovarian cancer is younger among women with a hereditary ovarian cancer syndrome. The risk of ovarian cancer reaches 2%–3% in women with a BRCA1 gene mutation at age 35 and for those with a BRCA2 mutation at age 50.[6] [7]
Linkage analysis of familial breast and ovarian cancers provided some of the first insights into the molecular basis of ovarian cancer. These efforts ultimately identified two gene products, BRCA 1 and BRCA2, each clearly associated with an increased incidence of ovarian cancer. The estimated lifetime risk of ovarian cancer is 35%–46% for BRCA1 mutation carriers and 13%–23% for BRCA2 mutation carriers.[8]
Women with BRCA1 gene mutations typically develop ovarian cancer at an earlier age than other women, with an average age at diagnosis of 50-year-old and a 2%–3% incidence of ovarian cancer by age of 40 years.[6] [7] The average age at diagnosis of ovarian cancer in BRCA2 mutation carriers is 60-year-old, similar to the general population; women with this mutation reach an incidence of 2%–3% by 50-year-old.
The stage at presentation of ovarian cancer is similar for BRCA carriers and the general population; approximately 70% of patients present with Stage III or IV disease.[9] However, ovarian cancers in BRCA mutation carriers are more likely to be of higher grade than ovarian cancers in age-matched controls. BRCA1 and 2 carriers with ovarian cancer appear to have a similar distribution of histologic types to the general population. Serous adenocarcinoma is the most common histopathology phenotype; mucinous or borderline histology is rare.[9]
BRCA mutation carriers, particularly BRCA2 carriers, appear to have a better prognosis than noncarriers. This was best illustrated in a meta-analysis of 26 observational studies including over 3000 women that found the following stage, grade, and histology-adjusted 5-year all-cause mortality rates. This improved survival appears to be due to a higher sensitivity of platinum-based treatment of these tumors relative to sporadic cases, which is maintained across repeated courses of chemotherapy.[10] [11] [12] [13]
A BRCA gene mutation is the most established risk factor for fallopian tubal and peritoneal carcinoma. BRCA mutation carriers rarely present with a tumor that is recognized as a primary tubal cancer (0.6% lifetime incidence). BRCA mutations, primarily BRCA1, have been identified in 16%–43% of women with fallopian tubal cancer.[14] [15] [16] Therefore, BRCA mutation testing should be offered to women with these tumors, and risk-reduction surgery for BRCA carriers includes salpingectomy.
The frequency of BRCA 1 and 2 mutations in Indian population is largely unknown. Various studies have quoted different figures. In this study, we have tried to correlate clinicoepidemiological profile of BRCA mutations with that of nonmutated.
Aim and objective
The aim of this study is to study the incidence, clinical profile, and outcomes of a patient with BRCA 1 and BRCA 2 mutation in carcinoma ovary and its comparison with patients without mutation.
Inclusion criterion
As per latest existent guidelines National Comprehensive Cancer Network (NCCN) Guideline version 2.2015 (National Cancer Institute, USA) all the patients with personal history of Invasive Epithelial Ovarian Cancer were included in the study. Patients were explained about the genetic testing, and only those who are willing for the test were included in the study.
Exclusion criteria
All patients with nonepithelial cancer or not fulfilling the inclusion criteria or not willing for genetic testing due to any reasons were not included.
Materials and Methods
This study was an observational and prospective study. The patient was recruited from both out-patient and in-patient departments of the Department of Medical Oncology of the Army Hospital (Research and Referral), New Delhi. Our target study population included serving armed forces personnel, their dependents, and retired serving personnel fulfilling the inclusion and exclusion criteria.
Totally, 50 patients fulfilling the inclusion criteria were included in the study. A detailed history, relevant clinical examination, and appropriate investigations were done for each patient. They received treatment as per the existing guidelines and were followed up at 3, 6, 9, months after treatment and were assessed as per the RECIST criteria (ver 1.1).
Every patient was subjected to BRCA 1 and BRCA 2 mutational analysis by Next Generation Sequence Analysis (Whole Genome Sequencing) of the peripheral blood after due genetic counseling and due informed consent of the patient. Based on the results, patients were divided into two groups, i.e., the patient having BRCA mutation and patients without BRCA mutation.
Institutional Review Board and Ethical Committee reviewed the study, and no observations were raised.
Results
In the study, 50 patients of carcinoma Ovary and who were eligible for BRCA mutational studies. These patients were further subdivided into two groups, namely (a) patients who are BRCA negative and (b) patients who are BRCA mutation positive. Various characteristics were compared for the two groups.
Out of total 50 patients, 45 (90%) were BRCA negative and rest five (10%) were BRCA positive. Of the five patients, only two (4% of total) had pathological mutations while the rest of three patients had benign mutations only [Table 1].
Table 1Types of BRCA mutations in carcinoma ovary
|
Mutations detected |
Pathogenic or benign |
Number of patients |
|---|---|---|
|
BRCA1: c.1961delA |
Pathogenic |
01 |
|
BRCA1: c.5251C>T |
Pathogenic |
01 |
|
BRCA1c.2350A>G |
Benign |
03 |
Out of total 50 patients of carcinoma ovary, most of the patients were of the age >60 years (23 out of 50, i.e., 46%), while 38% (19 out of 50) were in the age group of 40–60 years while the number of young patients ( < 40) were only 16% (8 out of 50). Overall median age of presentation was 61 years for BRCA-negative patients and 38 years for BRCA-positive patients.
While those patients who were BRCA negative most common age of presentation was >60 years (23 out of 45:51.1%) but for BRCA-positive patient the age of presentation was detected to be earlier i.e., < 40 years (3 out of 05; 60%) and rest of the patient also presented at earlier age as compare to BRCA-negative patients. Both patients with pathological mutations were < 40 years of age [Table 2] and [Figure 1].
Table 2
Age-wise distribution in carcinoma ovary
|
Age |
BRCA negative |
BRCA positive |
Total number of patients |
|---|---|---|---|
|
less than 40 |
05 |
03 |
08 |
|
40-60 |
17 |
02 |
19 |
|
>60 |
23 |
0 |
23 |
| Fig. 1 Age-wise distribution in carcinoma ovary
Overall, the most common presentation in our study was dyspepsia (80%), and abdominopelvic mass was the second-most common complaint for 38 out of 50 patients (76%). Other common presentations in our study were ascites which was present in 29 out of 50 patients (58%), pain (30%), anorexia (38%), pleural effusion (14%), bony pain (6%), CNS manifestations (4%), and significant weight loss in 16% of the patients.
BRCA-positive patients also followed the BRCA-negative patients in term of clinical presentation. The most common presentation was abdominopelvic lump (04 out of 05: 80%) while other common presentations were ascites (60%) and anorexia (60%). Both the patients with pathological mutations presented with abdominopelvic lump and ascites [Table 3] and [Figure 2].
Table 3 Various clinical manifestations in carcinoma ovary
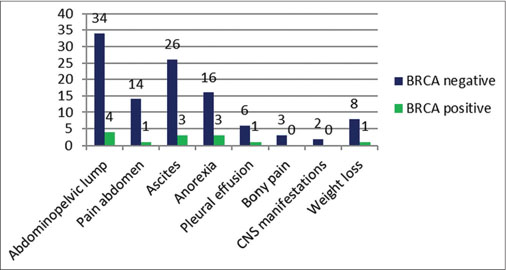
| Fig. 2 Various clinical manifestations in carcinoma ovary
Detailed family history was taken from all the patients, and eight patients gave significant family history (16%). While 100% of the BRCA-positive patients had significant family history as compare to only three patients who were BRCA negative (6.7%). Out of these patients, five had a history of the first-degree relative being affected (62.5%) out of which four were BRCA positive including two with pathological mutations while three (37.8%) had a history of second degree relative being affected including one with nonpathological mutation [Table 4] and [Figure 3].
Family history in carcinoma ovary
|
Degree of relative |
BRCA positive |
BRCA negative |
Number of patients |
|---|---|---|---|
|
First degree |
04 |
01 |
05 |
|
Second degree |
01 |
02 |
03 |
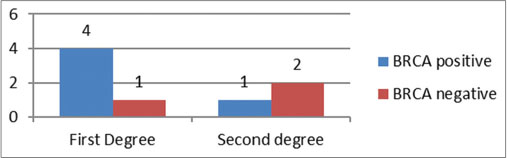
| Fig. 3 Family history in carcinoma ovary
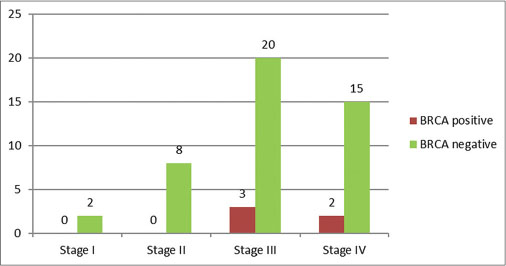
Most of the patients presented in Stage III (23 out of 50; 46%), while the second-most common presentation was in Stage IV (34%). For patients who were BRCA negative most common stage of presentation was also Stage III (20 out of 45; 44.4%) while second-most common presentation was in Stage IV. However, in BRCA-positive subgroup, although the most common presentation was also in Stage III (60%) both the patients who were BRCA positive with pathological mutation presented in Stage IV (40%). Hence, Stage IV was more common presentation for patients with pathological mutation [Table 5] and [Figure 4].
Stage-wise distribution in carcinoma ovary
|
Stage |
BRCA positive |
BRCA negative |
Number of patients |
|---|---|---|---|
|
Stage I (including IA, IB, and IC) |
00 |
02 |
02 |
|
Stage II (including IIA, IIB, and IIC) |
00 |
08 |
08 |
|
Stage III (including IIIA, IIIB, and IIIC) |
03 |
20 |
23 |
|
Stage IV |
02 |
15 |
17 |
| Fig. 4 Stage-wise distribution in carcinoma ovary
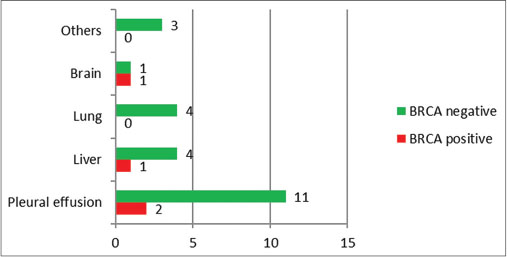
Seventeen patients presented with metastatic disease out of total 50 patients (34%). In our study, we found that the pleural effusion was the most common site of metastasis (76.4%) while the liver being the second most site (29.4%). Clinically, only 07 patients were detected to have pleural effusion as mentioned in [Table 3]. However, on further investigation, 13 patients were detected to have metastatic pleural effusion. Two patients who were BRCA positive had pleural effusion in both the patients. Other sites were liver and brain [Table 6] and [Figure 5].
Sites of metastasis in carcinoma ovary
|
Sites of metastasis |
BRCA positive |
BRCA negative |
Number of patients |
|---|---|---|---|
|
Pleural effusion |
02 |
11 |
13 |
|
Liver |
01 |
04 |
05 |
|
Lung |
00 |
04 |
04 |
|
Brain |
01 |
01 |
02 |
|
Others |
00 |
03 |
03 |
| Fig. 5 Sites of metastasis in carcinoma ovary
The patients were reassessed after completion of planned treatment. Stage-wise response assessment was done. For Stage I and II, all the patients achieved complete response (CR) after completion of treatment (100%), while for patients in Stage III 21 out of 23 patients (91.3%) achieved CR while 2 had residual disease (8.6%). In Stage IV patients, 11 out of 17 (64.7%) achieved CR, and 6 patients had residual disease (35.2%). Out of all five BRCA-positive patients, overall 100% were able to achieve CR on platinum-based therapy while for the patients who were BRCA negative only 75.5% (34 out of 45) were able to achieve CR [Table 7] and [Figures 6], [7].
Table 7 Response assessment in carcinoma ovary
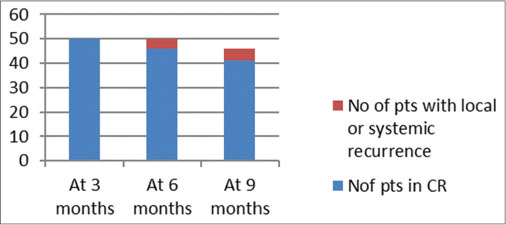
| Fig. 6 Response assessment in carcinoma ovary
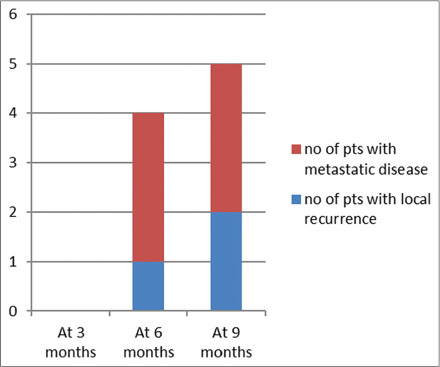
| Fig. 7 Type of recurrence in carcinoma ovary
Rest of the remaining 42 patients were followed up at 3, 6, and 9 months. On follow-up, they were evaluated with a detailed history and clinical examination and relevant investigations.
On reassessment at 3 months, 3 out of 42 patients had recurrence (7.1%). All of the patients were BRCA negative and were initially staged as Stage IV. Recurrence was most commonly associated with ascites (100%), two patients presented with pelvic mass (66.7%), one patient had brain metastasis (33%). None of the BRCA-positive patients had recurrence at 3 months.
At 6 months, out of the remaining 39 patients, 5 patients recurred (12.8%). All of the patients were BRCA negative. Three patients were in Stage III and rest of the two was in Stage IV. In this subgroup also, the ascites was the most common presentation (4 out of 5; 80%) other common presentations were pelvic mass, liver metastasis, pleural effusion, and lung metastasis.
At 9 months, out of the remaining 34 patients who were in CR, 29 remained in CR only. There were 5 patients who had recurrence. Four patients were BRCA negative and one patient was BRCA positive with nonpathological mutation. Three patients were in Stage III and rest of the two was in Stage IV. In this subgroup also, the ascites was the most common presentation (4 out of 5; 80%) other common presentations were pelvic mass, liver metastasis, pleural effusion, and lung metastasis.
In our study, we had an overall mortality of one patient who was BRCA negative, in Stage IV while no mortality was noted in BRCA positive subset of patients.
Discussion
Ovarian cancer is the second most common cancer (age standardized incidence rate: 6.6/100,000) and the seventh leading cause of cancer deaths (age standardized mortality rate: 4.0/100,000) among women worldwide.[17] [18] In most of the population-based cancer registries in India, ovarian cancer is the third leading site of cancer among women, trailing behind cervix, and breast cancer.
The PBCRs at Bengaluru (APC: 2.04%), Bhopal (2.38%), Chennai (1.56%), Delhi (0.98%), and Mumbai (0.86%) showed a statistically significant increase in the occurrence of ovarian cancers over time. All the PBCRs except for Bhopal showed a significant increase for annual average of average annual returns for both 3 and 5 years whereas Bhopal showed an increase in 3 years trend.[17]
Epidemiologic studies indicate that hereditary cancers constitute 5%–10% of all epithelial ovarian cancers. These cancers are autosomal dominant conferred primarily by mutations in BRCA1 and BRCA2 genes.[18] Estimates of the frequency of BRCA1 and BRCA2 germline mutations in ovarian cancer have ranged between 2%–12% and 2%–6% for BRCA1 and BRCA2 mutations, respectively.[19] However, in our study, only 4% of the patients were detected to have pathological BRCA mutations.
Women with BRCA1 gene mutations typically develop ovarian cancer at an earlier age than other women, with an average age at diagnosis of 50-year-old and a 2%–3% incidence of ovarian cancer by the age of 40 years. The average age at diagnosis of ovarian cancer in BRCA2 mutation carriers is 60-year-old, similar to the general population; women with this mutation reach an incidence of 2%–3% by 50 years old.[20]
The stage at presentation of ovarian cancer is similar for BRCA carriers and the general population; approximately 70% of patients present with Stage III or IV disease.[9] However, ovarian cancers in BRCA mutation carriers are more likely to be of higher grade than ovarian cancers in age-matched controls.[20] BRCA1 and 2 carriers with ovarian cancer appear to have a similar distribution of histologic types to the general population. Serous adenocarcinoma is the most common histopathology phenotype; mucinous or borderline histology is rare.[9] [21]
BRCA mutation carriers, particularly BRCA2 carriers, appear to have a better prognosis than noncarriers. This was best illustrated in a meta-analysis of 26 observational studies including over 3000 women that found the following stage, grade, and histology-adjusted 5-year all-cause mortality rates:[22]
BRCA1 carriers versus noncarriers: 45 versus 47%; HR 0.73, 95% CI 0.64-0.84
BRCA2 carriers versus noncarriers: 36 versus 47%; HR 0.49, 95% CI 0.39-0.61.
This improved survival appears to be due to a higher sensitivity of platinum-based treatment of these tumors relative to sporadic cases, which is maintained across repeated courses of chemotherapy.[10]
The average age at diagnosis for sporadic tumors was 62.3 years, and that of familial cases was 49–54.3 years as reported by Zweemer et al. However, in our study, we observed that the mean age at diagnosis was 57.6 years for BRCA-negative patients while all patients who were BRCA positive were < 40 years of age. This was lower than the average age at diagnosis of 57 years for sporadic cases, 53 years for BRCA1, and 58 years for BRCA2 carriers as reported by Pal et al.[9] Thus the average age at presentation was lower in our study.
Saini et al. published 136 cases primary ovarian epithelial neoplasia were analyzed. For epithelial ovarian malignancy, patients’ mean age at diagnosis was 55.98 ± 9.24 (median = 55). Serous adenocarcinoma (49.69%) was the most prevalent type of histopathology followed by endometrioid (19.1%), mucinous (10.42%), and clear cell (4.29%). Dyspepsia, defined as burning, gnawing discomfort, or constellation of symptoms including postprandial fullness, early satiety (an inability to complete a meal due to premature fullness), bloating, and eructation (belching), were most commonly observed complaint (66.26%) of patients who later on diagnosed with malignant ovarian tumor. Abdominal lump or abdominal distension, pain in abdomen, urinary symptom, respiratory symptom, constipation, discharge/bleeding P/V, nausea/vomiting, and weakness were other observed symptoms.[9] [23]
In our study also, the most common presentation was dyspepsia, and the second-most common presentation was abdominal distension only. However, in the above study, it was not correlated with BRCA status. While the most common presentation was in Stage III for both subsets of patients.
After extensive literature search, our study was a unique study in the sense that role of BRCA mutations has not been evaluated in Indian setting. This was a single center-based and spanned over 24 months involving limited number of patients with ovarian cancer with maximum follow-up for 9 months. However, a multi-centric large population-based study with longer follow-up will be able to give a better picture in Indian scenario. In this study, very small number of patients was evaluated hence long-term studies will definitely provide better information about Indian patients. BRCA mutational studies were outsourced with funding limitations. Our patients presented at an early age with significant positive family history and sizeable number of them presented with triple-negative status pointing toward genetic association with BRCA1; hence, all such patients should be evaluated for BRCA 1 and 2 mutations. Apart from BRCA 1 and 2 mutations, there are many other genetic mutations which could be contributing to the disease hence these should also be studied. The so-called benign BRCA mutations should also be evaluated in Indian setting.
Conclusion
This was a single center-based study spanned over 24 months involving limited number of patients with ovarian cancer with maximum follow-up for 9 months. However, a multi-centric large population-based study with longer follow-up will be able to give a better picture in Indian scenario. In this study, very small number of patients was evaluated hence long-term studies will defi nitely provide better information about Indian patients.
Conflict of Interest
There are no conflicts of interest.
References
- 1 Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. et al. Global cancer statistics. CA Cancer J Clin 2011; 61: 69-90
- 2 Siegel R, Ma J, Zou Z, Jemal A. Cancer statistics, 2014. CA Cancer J Clin 2014; 64: 9-29
- 3 Available from: http://www.seer.cancer.gov/statfacts/html/ovary.html. [Last accessed on 2012 Apr 24]
- 4 Lacey JV, Sherman ME. Ovarian neoplasia. In: Robboy SL, Mutter GL, Prat J. editors Robboy’s Pathology of the Female Reproductive Tract. 2nd ed. Oxford: Churchill Livingstone Elsevier; 2009: 601
- 5 Berek JS, Crum C, Friedlander M. Cancer of the ovary, fallopian tube, and peritoneum. Int J Gynaecol Obstet 2012; 119 (02) Suppl S118-29
- 6 King MC, Marks JH, Mandell JB. New York Breast Cancer Study Group. Breast and ovarian cancer risks due to inherited mutations in BRCA1 and BRCA2. Science 2003; 302: 643-6
- 7 Satagopan JM, Boyd J, Kauff ND, Robson M, Scheuer L, Narod S. et al. Ovarian cancer risk in Ashkenazi Jewish carriers of BRCA1 and BRCA2 mutations. Clin Cancer Res 2002; 8: 3776-81
- 8 Chen S, Parmigiani G. Meta-analysis of BRCA1 and BRCA2 penetrance. J Clin Oncol 2007; 25: 1329-33
- 9 Pal T, Permuth-Wey J, Betts JA, Krischer JP, Fiorica J, Arango H. et al. BRCA1 and BRCA2 mutations account for a large proportion of ovarian carcinoma cases. Cancer 2005; 104: 2807-16
- 10 Bolton KL, Chenevix-Trench G, Goh C, Sadetzki S, Ramus SJ, Karlan BY. et al. Association between BRCA1 and BRCA2 mutations and survival in women with invasive epithelial ovarian cancer. JAMA 2012; 307: 382-90
- 11 Taniguchi T, Tischkowitz M, Ameziane N, Hodgson SV, Mathew CG, Joenje H. et al. Disruption of the Fanconi anemia-BRCA pathway in cisplatin-sensitive ovarian tumors. Nat Med 2003; 9: 568-74
- 12 Cass I, Baldwin RL, Varkey T, Moslehi R, Narod SA, Karlan BY. et al. Improved survival in women with BRCA-associated ovarian carcinoma. Cancer 2003; 97: 2187-95
- 13 Tan DS, Rothermundt C, Thomas K, Bancroft E, Eeles R, Shanley S. et al. “BRCAness” syndrome in ovarian cancer: A case-control study describing the clinical features and outcome of patients with epithelial ovarian cancer associated with BRCA1 and BRCA2 mutations. J Clin Oncol 2008; 26: 5530-6
- 14 Levine DA, Argenta PA, Yee CJ, Marshall DS, Olvera N, Bogomolniy F. et al. Fallopian tube and primary peritoneal carcinomas associated with BRCA mutations. J Clin Oncol 2003; 21: 4222-7
- 15 Aziz S, Kuperstein G, Rosen B, Cole D, Nedelcu R, McLaughlin J. et al. A genetic epidemiological study of carcinoma of the fallopian tube. Gynecol Oncol 2001; 80: 341-5
- 16 Cass I, Holschneider C, Datta N, Barbuto D, Walts AE, Karlan BY. et al. BRCA-mutation-associated fallopian tube carcinoma: A distinct clinical phenotype?. Obstet Gynecol 2005; 106: 1327-34
- 17 Pennington KP, Swisher EM. Hereditary ovarian cancer: Beyond the usual suspects. Gynecol Oncol 2012; 124: 347-53
- 18 Prevalence and penetrance of BRCA1 and BRCA2 mutations in a population-based series of breast cancer cases. Anglian Breast Cancer Study Group. Br J Cancer 2000; 83: 1301-8
- 19 Indian Council of Medical Research. Consolidated Report of Population Based Cancer Registries 2012-2014. Bangalore: Indian Council of Medical Research; 2014
- 20 Boyd J, Sonoda Y, Federici MG, Bogomolniy F, Rhei E, Maresco DL. et al. Clinicopathologic features of BRCA-linked and sporadic ovarian cancer. JAMA 2000; 283: 2260-5
- 21 Lakhani SR, Manek S, Penault-Llorca F, Flanagan A, Arnout L, Merrett S. et al. Pathology of ovarian cancers in BRCA1 and BRCA2 carriers. Clin Cancer Res 2004; 10: 2473-81
- 22 Piver MS. Hereditary ovarian cancer. Lessons from the first twenty years of the Gilda Radner familial ovarian cancer registry. Gynecol Oncol 2002; 85: 9-17
- 23 Saini SK, Srivastava S, Singh Y. Epidemiology of epithelial ovarian cancer, a single institution-based study in India. Clini Cancer Investig J 2016; 5: 20-4
Address for correspondence
Dr. S VishwanathDepartment of Medical Oncology, Army Hospital (R and R)New Delhi - 110 010IndiaEmail: drsonikrathore@gmail.comPublication History
Received: 25 March 2018
Accepted: 21 June 2018
Article published online:
03 June 2021© 2020. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
| Fig. 1 Age-wise distribution in carcinoma ovary
| Fig. 2 Various clinical manifestations in carcinoma ovary
| Fig. 3 Family history in carcinoma ovary
| Fig. 4 Stage-wise distribution in carcinoma ovary
| Fig. 5 Sites of metastasis in carcinoma ovary
| Fig. 6 Response assessment in carcinoma ovary
| Fig. 7 Type of recurrence in carcinoma ovary
References
- 1 Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. et al. Global cancer statistics. CA Cancer J Clin 2011; 61: 69-90
- 2 Siegel R, Ma J, Zou Z, Jemal A. Cancer statistics, 2014. CA Cancer J Clin 2014; 64: 9-29
- 3 Available from: http://www.seer.cancer.gov/statfacts/html/ovary.html. [Last accessed on 2012 Apr 24]
- 4 Lacey JV, Sherman ME. Ovarian neoplasia. In: Robboy SL, Mutter GL, Prat J. editors Robboy’s Pathology of the Female Reproductive Tract. 2nd ed. Oxford: Churchill Livingstone Elsevier; 2009: 601
- 5 Berek JS, Crum C, Friedlander M. Cancer of the ovary, fallopian tube, and peritoneum. Int J Gynaecol Obstet 2012; 119 (02) Suppl S118-29
- 6 King MC, Marks JH, Mandell JB. New York Breast Cancer Study Group. Breast and ovarian cancer risks due to inherited mutations in BRCA1 and BRCA2. Science 2003; 302: 643-6
- 7 Satagopan JM, Boyd J, Kauff ND, Robson M, Scheuer L, Narod S. et al. Ovarian cancer risk in Ashkenazi Jewish carriers of BRCA1 and BRCA2 mutations. Clin Cancer Res 2002; 8: 3776-81
- 8 Chen S, Parmigiani G. Meta-analysis of BRCA1 and BRCA2 penetrance. J Clin Oncol 2007; 25: 1329-33
- 9 Pal T, Permuth-Wey J, Betts JA, Krischer JP, Fiorica J, Arango H. et al. BRCA1 and BRCA2 mutations account for a large proportion of ovarian carcinoma cases. Cancer 2005; 104: 2807-16
- 10 Bolton KL, Chenevix-Trench G, Goh C, Sadetzki S, Ramus SJ, Karlan BY. et al. Association between BRCA1 and BRCA2 mutations and survival in women with invasive epithelial ovarian cancer. JAMA 2012; 307: 382-90
- 11 Taniguchi T, Tischkowitz M, Ameziane N, Hodgson SV, Mathew CG, Joenje H. et al. Disruption of the Fanconi anemia-BRCA pathway in cisplatin-sensitive ovarian tumors. Nat Med 2003; 9: 568-74
- 12 Cass I, Baldwin RL, Varkey T, Moslehi R, Narod SA, Karlan BY. et al. Improved survival in women with BRCA-associated ovarian carcinoma. Cancer 2003; 97: 2187-95
- 13 Tan DS, Rothermundt C, Thomas K, Bancroft E, Eeles R, Shanley S. et al. “BRCAness” syndrome in ovarian cancer: A case-control study describing the clinical features and outcome of patients with epithelial ovarian cancer associated with BRCA1 and BRCA2 mutations. J Clin Oncol 2008; 26: 5530-6
- 14 Levine DA, Argenta PA, Yee CJ, Marshall DS, Olvera N, Bogomolniy F. et al. Fallopian tube and primary peritoneal carcinomas associated with BRCA mutations. J Clin Oncol 2003; 21: 4222-7
- 15 Aziz S, Kuperstein G, Rosen B, Cole D, Nedelcu R, McLaughlin J. et al. A genetic epidemiological study of carcinoma of the fallopian tube. Gynecol Oncol 2001; 80: 341-5
- 16 Cass I, Holschneider C, Datta N, Barbuto D, Walts AE, Karlan BY. et al. BRCA-mutation-associated fallopian tube carcinoma: A distinct clinical phenotype?. Obstet Gynecol 2005; 106: 1327-34
- 17 Pennington KP, Swisher EM. Hereditary ovarian cancer: Beyond the usual suspects. Gynecol Oncol 2012; 124: 347-53
- 18 Prevalence and penetrance of BRCA1 and BRCA2 mutations in a population-based series of breast cancer cases. Anglian Breast Cancer Study Group. Br J Cancer 2000; 83: 1301-8
- 19 Indian Council of Medical Research. Consolidated Report of Population Based Cancer Registries 2012-2014. Bangalore: Indian Council of Medical Research; 2014
- 20 Boyd J, Sonoda Y, Federici MG, Bogomolniy F, Rhei E, Maresco DL. et al. Clinicopathologic features of BRCA-linked and sporadic ovarian cancer. JAMA 2000; 283: 2260-5
- 21 Lakhani SR, Manek S, Penault-Llorca F, Flanagan A, Arnout L, Merrett S. et al. Pathology of ovarian cancers in BRCA1 and BRCA2 carriers. Clin Cancer Res 2004; 10: 2473-81
- 22 Piver MS. Hereditary ovarian cancer. Lessons from the first twenty years of the Gilda Radner familial ovarian cancer registry. Gynecol Oncol 2002; 85: 9-17
- 23 Saini SK, Srivastava S, Singh Y. Epidemiology of epithelial ovarian cancer, a single institution-based study in India. Clini Cancer Investig J 2016; 5: 20-4