 PDF
PDF  Views
Views  Share
Share


Effect of areca nut chewing and maximal mouth opening in schoolgoing children in Ahmedabad
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2016; 37(04): 239-241
DOI: DOI: 10.4103/0971-5851.195734
Abstract
Context: Areca nut is chewed by itself and in various scented preparations. Areca nut chewing is widely practiced in many parts of Asia, including India. Users often consider it harmless and report a sense of well-being, but evidence has shown that it is far from harmless and can have multiple oral health implications such as oral submucosal fibrosis posing difficulty in opening mouth and carcinogenesis. Studies in India have reported increasing prevalence of this habit among schoolgoing children. The objectives of the study were to find the effect of areca nut chewing on mouth opening, compare it with the children not having this habit, and to find correlation between maximal mouth opening (MMO) and months of areca nut chewing. Aims: The aim of this study is to find the effect of areca nut chewing on MMO in schoolgoing children in Ahmedabad. Settings and Design: An observational analytical study was conducted across various schools of Ahmedabad. Subjects and Methods: A total of eighty male students of 12–14-year-old were included in the study. Group A included children having the habit of eating areca nut for 6 months or more, and Group B had children who did not have the habit of areca nut chewing. Children who had just started eating for < 6 months were excluded from the study. MMO was calculated as distance from the edge of the upper incisor teeth to the edge of the lower incisor teeth using a calibrated fiber ruler. Statistical Analysis Used: Statistical analysis was performed by SPSS software version 20.0, with level of significance set at 5%. Results: Mean and standard deviation of MMO for Group A was 3.69 ± 0.5 cm and for Group B was 4.46 ± 0.4 cm. Statistically significant difference was found using Mann–Whitney U-test with U = 239.500 and P = 0.0001. Pearson's coefficient r = −0.623 and P = 0.0001 showed moderate correlation between months of chewing and MMO. The mean duration of chewing was found to be 1.5 years. Conclusion: There is difference in MMO between children chewing areca nut and not chewing it with a moderate correlation between months of eating areca nut and MMO.
Publication History
Article published online:
12 July 2021
© 2016. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Abstract
Context:
Areca nut is chewed by itself and in various scented preparations. Areca nut chewing is widely practiced in many parts of Asia, including India. Users often consider it harmless and report a sense of well-being, but evidence has shown that it is far from harmless and can have multiple oral health implications such as oral submucosal fibrosis posing difficulty in opening mouth and carcinogenesis. Studies in India have reported increasing prevalence of this habit among schoolgoing children. The objectives of the study were to find the effect of areca nut chewing on mouth opening, compare it with the children not having this habit, and to find correlation between maximal mouth opening (MMO) and months of areca nut chewing.
Aims:
The aim of this study is to find the effect of areca nut chewing on MMO in schoolgoing children in Ahmedabad.
Settings and Design:
An observational analytical study was conducted across various schools of Ahmedabad.
Subjects and Methods:
A total of eighty male students of 12–14-year-old were included in the study. Group A included children having the habit of eating areca nut for 6 months or more, and Group B had children who did not have the habit of areca nut chewing. Children who had just started eating for < 6 months were excluded from the study. MMO was calculated as distance from the edge of the upper incisor teeth to the edge of the lower incisor teeth using a calibrated fiber ruler.
Statistical Analysis Used:
Statistical analysis was performed by SPSS software version 20.0, with level of significance set at 5%.
Results:
Mean and standard deviation of MMO for Group A was 3.69 ± 0.5 cm and for Group B was 4.46 ± 0.4 cm. Statistically significant difference was found using Mann–Whitney U-test with U = 239.500 and P = 0.0001. Pearson's coefficient r = −0.623 and P = 0.0001 showed moderate correlation between months of chewing and MMO. The mean duration of chewing was found to be 1.5 years.
Conclusion:
There is difference in MMO between children chewing areca nut and not chewing it with a moderate correlation between months of eating areca nut and MMO.
INTRODUCTION
Areca nut (supari) is chewed by itself and in various scented preparations. Areca nut chewing is widely practiced in many parts of Asia, including India.[1] Studies in India have reported increasing prevalence of this habit among schoolgoing children.[1,2,3] Krishna D et al. in their study on the prevalence and characteristics of areca nut, gutka, and tobacco among schoolchildren of rural areas in and around Gandhinagar found 33.33% and 22.28% of the prevalence among male and female students, respectively.[1] Users often consider it harmless and report a sense of well-being, but evidence has shown that it is far from harmless and can have multiple oral health implications such as oral submucosal fibrosis (OSMF) posing difficulty in opening mouth and carcinogenesis.[4]
The objectives of the study were to find the effect of areca nut chewing on mouth opening, compare it with the children not having this habit, and to find correlation between maximal mouth opening (MMO) and months of areca nut chewing.
SUBJECTS AND METHODS
An observational analytical study was conducted in two municipal schools of Ahmedabad, among 12–14-year-old male schoolgoing children. Group A included forty children having the habit of eating areca nut for 6 months or more, and Group B included forty children who did not have the habit of areca nut chewing. Children who had just started eating for < 6 months were excluded from the study. A total of eighty children were included using a convenient sampling design.
Permission for data collection was sought from the principals of the schools. Oral informed consent of the children included in the study was taken. Demographic data were collected using a self-made questionnaire. MMO was measured. For measuring MMO, children were asked to open their mouth fully till no further opening was possible. Average of three readings was taken. Distance from the edge of the upper incisor teeth to the edge of the lower incisor teeth was measured. A calibrated ruler was used for measurement.[5] Level of significance was kept at 5%.
Between-groups analysis was done using Mann–Whitney test. Correlation between months of eating and MMO was found using Spearman's correlation analysis.
RESULTS
Mean MMO was compared for Group A and Group B; the difference in mean MMO for Group A and Group B was found to be statistically significant. Comparison of mean MMO and SD of Group A and Group B is shown in Table 1. Correlation between months of chewing and MMO was done using Spearman's correlation as shown in Graph 1. A moderate negative correlation (r = −0.623) was found between months of areca nut chewing and MMO. The mean duration of areca nut was found to be 1.5 years.
Table 1
Comparison of mean maximal mouth opening and standard deviation of Group A and Group B

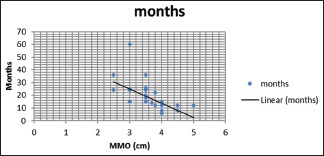
| Graph 1 Correlation of months of areca nut chewing and maximal mouth opening
DISCUSSION
The mean MMO was found to be significantly reduced in children who had the habit of chewing areca nut (3.69 cm) than those who did not have the habit (4.46 cm).
MMO for Indian boys is 4.6 cm, 4.8 cm, and 5.2 cm in age groups of 6–8, 8–10, and 10–12 years, respectively.[5] It is seen that as age increase mouth opening increases. The MMO in the present study was less than above findings even though age group was slightly more.
Furthermore, a moderate correlation was found between months of chewing areca nut and MMO. Reddy et al. in their study on correlation of the clinical grading of OSMF to various chewing habits found that the relative risk of OSMF increased with duration, frequency, and style of chewing habits for longer duration, which is similar to the present findings.[6] Nigam et al. in their study on 1000 individuals having habit of chewing nut or gutka for 1 year or more found the prevalence of OSMF to be 6.3%. Out of which 58.7% individuals had reduced mouth opening with MMO of < 3 cm and 38.09% had altered taste sensations.[7]
Dere et al. in their study on the prevalence and characteristics of areca nut, gutka, and tobacco among schoolchildren of rural areas in and around Gandhinagar found 10% boys and 2% females to be suffering with OSMF with reduction in MMO.[1] Gupta et al. in their study on series of two cases, one girl aged 11 years and eating areca nut for 7 years and other boy aged 10 years and eating areca nut since 6 years, showed that both had complaints of reduced mouth opening, discomfort, and burning sensation particularly when eating spicy food found MMO to be 1.4 cm and 1.3 cm, respectively.[8] Reduced mouth opening was more than seen in the present study probably because duration of eating was maximum 3 years.
The major chemical constituents of areca nut are carbohydrates, fats, and alkaloids.[9] Arecoline, one of the alkaloids, is the main agent for carcinogenic effect.[10] Application of these substances to human fibroblasts induces fibroblastic proliferation and collagen production and thus progressive difficulty in mouth opening leading to OSMF.[11] OSMF is a premalignant condition of oral cavity strongly associated with nut and gutka chewing. It is characterized by burning sensation of mouth especially while eating spicy food, fibrosis of oral soft tissue resulting in decreased mouth opening, and pallor of oral mucosa.[12] The present study, however, did not evaluate the other above characteristics.
The malignant transformation rate of OSMF has been found to be 13%–40% worldwide, whereas it is 7.6% in the Indian population.[13] Goel et al. studied OSMF by dividing 100 cases into three stages; Stage 1 – MMO >4.1 cm, Stage 2 – restricted MMO 2–4.4 cm, and Stage 3 MMO < 2 cm. They found that 60% of individuals had restricted MMO falling into Stage 2.[14]
It is likely that children who are regular chewers at early age will be dependent on the nut and continue the chewing habit in their adult life, which will make them more prone to OSMF, unless appropriate intervention is made.[8]
Only boys were included in the study which is one of the limitations of the study.
The collected data can be used for the purpose of planning areca nut chewing control interventions and evaluation. Studies to see effect of exercises on MMO in OSMF need to be given proper emphasis.
CONCLUSION
There is difference in MMO between the children chewing areca nut and not chewing it. There is a correlation between months of eating areca nut and MMO.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
| Graph 1 Correlation of months of areca nut chewing and maximal mouth opening