 PDF
PDF  Views
Views  Share
Share


Effect of folate status and methylenetetrahydrofolate reductase genotypes on the complications and outcome of high dose methotrexate chemotherapy in north Indian children with acute lymphoblastic leukemia
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2016; 37(02): 85-89
DOI: DOI: 10.4103/0971-5851.180144
Abstract
Purpose: The genes of the folate metabolic pathway have been associated with toxicities during high dose methotrexate therapy for childhood ALL, however, the importance of intrinsic folate status in this regard is unclear. Methods: In the present study the effect of precourse folate levels and MTHFR genotypes on the complications during high dose methotrexate chemotherapy in children with ALL were examined. Results: Twenty-one children were studied. Folate deficiency was associated with higher incidence of neutropenia (P = 0.03) and longer duration of chemotherapy interruption (P = 0.009). Children with MTHFR1298 mutations needed more red cell transfusion (P = 0.03). All 3 deaths encountered were seen in folate deficient children. Conclusions: Folate deficiency was associated with higher complications during high dose methotrexate therapy, the implications of which are important especially in resource poor settings with high prevalence of folate deficiency.
Publication History
Article published online:
12 July 2021
© 2016. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Abstract
Purpose:
The genes of the folate metabolic pathway have been associated with toxicities during high dose methotrexate therapy for childhood ALL, however, the importance of intrinsic folate status in this regard is unclear.
Methods:
In the present study the effect of precourse folate levels and MTHFR genotypes on the complications during high dose methotrexate chemotherapy in children with ALL were examined.
Results:
Twenty-one children were studied. Folate deficiency was associated with higher incidence of neutropenia (P = 0.03) and longer duration of chemotherapy interruption (P = 0.009). Children with MTHFR1298 mutations needed more red cell transfusion (P = 0.03). All 3 deaths encountered were seen in folate deficient children.
Conclusions:
Folate deficiency was associated with higher complications during high dose methotrexate therapy, the implications of which are important especially in resource poor settings with high prevalence of folate deficiency.
INTRODUCTION
Methotrexate (Mtx), an antifolate drug is one of the most important agents used in the treatment of childhood acute lymphoblastic leukemia (ALL).[1] Though all children under treatment for ALL receive Mtx in one form or the other, a high-risk subset of these children receive higher doses of Mtx (>1000 mg/m2) during treatment.[2] Use of high dose Mtx (HD-Mtx) is associated with certain complications due to toxicity to normal cells, which can be largely ameliorated by the rescue of normal cells with folinic acid (leucovorin).[3] However, many of these toxicities cannot be totally eliminated despite the use of folinic acid.[2,3] The predictors of Mtx toxicity have been studied and include the dosage of Mtx used, the rescue dose of folinic acid[3] as well as mutations in certain genes involved in folate metabolism.[4] Mtx predominantly blocks folic acid metabolism in the cell and, therefore, intrinsic folic acid status should conceivably be a predictor of Mtx toxicity.[5] However, despite the high prevalence of folate deficiency in children in the developing countries and in countries without food fortification with folic acid, the role of intrinsic folate status of these children on the complications of HD-Mtx has not been studied till date.[5] The present study examines the impact of precourse folic acid status as well as methylenetetrahydrofolate reductase genotype on the complications and outcome of children undergoing HD-Mtx therapy.
METHODS
Among the children being treated for ALL in our unit between December 2011 and November 2013, those receiving HD-Mtx during interim maintenance (IM) phase of treatment were consecutively enrolled in the study. Fifteen children with proven T-ALL immunophenotype and another 6 without known immunophenotype, but very high initial TLC (>1 × 105 cells/mm3) at presentation received HD-Mtx during IM (4 doses of 3 g/m2 every 14 days). The dose of Mtx was followed by folinic acid rescue (30 mg/m2 folinic acid intravenously at 24 h of start of Mtx followed by 4 doses of 15 mg/m2 folinic acid every 6 hourly, and another 4 doses of 15 mg/m2 each at 12 h intervals). Patients also received oral 6-mercaptopurine on a daily basis for 49 days during this phase. They were monitored for the complications according to NCI common toxicity criteria version 4.03. They underwent regular investigations including routine counts and biochemistry at least before each dose of Mtx and 7 days thereafter. However, the frequency and extent of investigations were altered for individual patients depending upon their clinical condition. The study was approved by the institutional ethics committee of King George's Medical University, Lucknow.
Statistical analysis was performed using SPSS version 16.0 for Windows (Statistical Package for Social Sciences, SPSS Inc., USA) and GraphPad Prism® 3 (Version 3.0, GraphPad Software, Inc., USA). Descriptive statistics was used to compute central tendencies, dispersions, and frequencies. Intergroup comparisons between different methylenetetrahydrofolate reductase (MTHFR) genotypes as well as between children with normal folate and folate deficiency were done using Student's t-test for continuous variables and Mann-Whitney U-test for nonparametric data. Categorical variables were analyzed using Chi-square and Fischer's exact tests. Difference in survival between children with and without folate deficiency was computed by survival analysis using log-rank (Mantel-Cox) tests and presented as Kaplan-Meier curves. P < 0.05 were considered as statistically significant.
RESULTS
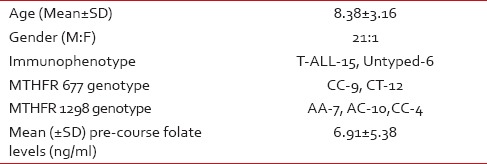
The baseline characteristics and the MTHFR genotypes of the children are as in Table 1. The mean precourse level of serum folate was 6.91 ± 5.38 ng/ml which underwent a modest decline to a mean level of 6.66 ± 4.34 after 4 doses of 2 weekly HD-Mtx. However, this difference was not statistically significant (P = 0.83; paired t-test).
Table 1
Baseline characteristics of the children who received HDMtx (n = 21)
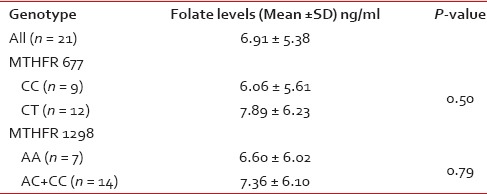
Though, the mean pretherapy folate levels were higher in MTHFR 677 wild (CC) genotype (7.89 ± 6.23 ng/ml) as compared to that in mutant (CT+TT) genotypes (6.06 ± 5.61 ng/ml), the difference did not reach statistical significance. Similarly, the difference of folate levels between the MTHFR 1298 wild (AA) genotype (7.36 ± 6.10 ng/ml) and the mutated (AC + CC) genotypes (6.60 ± 6.02 ng/ml) was also not statistically significant, despite showing same trend as in case of 677 genotypes [Table 2].
Table 2
Pre-methotrexate, folate levels and MTHFR genotypes
The effect of pretreatment folate status and the MTHFR genotypes on the complications and outcome of HD-Mtx therapy is presented in Table 3.
Table 3
Complications and outcome of high-dose methotrexate therapy in relation to folate status and MTHFR genotypes of children with ALL (n = 21)
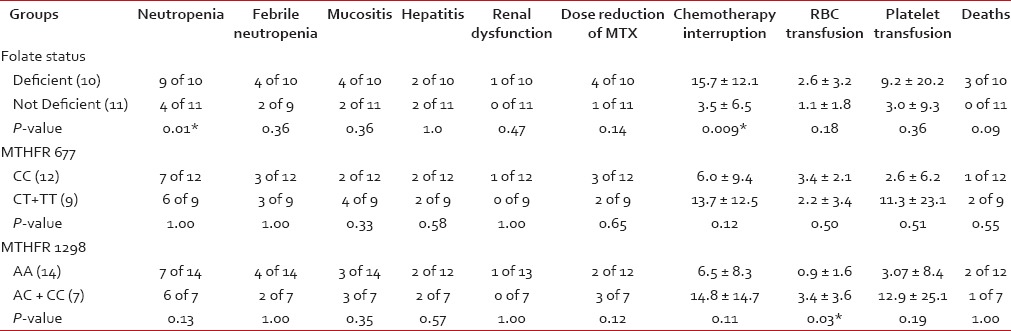 Folate deficiency seen in 10 of 21 children undergoing treatment was associated
with a significantly higher incidence of neutropenia during treatment (90% vs., 36%; P = 0.01) and a longer duration of chemotherapy interruption (15.7 ±
12.1 vs. 3.5 ± 6.5 days; P = 0.009). Three of 21
patients died due to sepsis induced by neutropenia during the phase of HD-Mtx. The incidence of toxic deaths was
much higher in children with folate deficiency as compared to normal folate status (30% vs. 0%; P = 0.09 - Fischer's exact test and 0.05 - Log rank test) [Figure 1]. Other complications like febrile neutropenia, mucositis,
renal dysfunction were also higher in children with folate deficiency but were not statistically significant.
Similarly, the transfusion requirements of folate deficient children were also higher as compared to
folate-sufficient children (packed red cell-2.6 ± 3.2 vs. 1.1 ± 1.8 units; P = 0.18, platelet concentrate 9.2 ± 20.2 vs. 3.0 ± 9.3 units; P = 0.36). Folate deficient children more often required a reduction in
the dose of Mtx in the subsequent cycles as compared to folate-sufficient children (40% vs. 9%; P = 0.14).
Folate deficiency seen in 10 of 21 children undergoing treatment was associated
with a significantly higher incidence of neutropenia during treatment (90% vs., 36%; P = 0.01) and a longer duration of chemotherapy interruption (15.7 ±
12.1 vs. 3.5 ± 6.5 days; P = 0.009). Three of 21
patients died due to sepsis induced by neutropenia during the phase of HD-Mtx. The incidence of toxic deaths was
much higher in children with folate deficiency as compared to normal folate status (30% vs. 0%; P = 0.09 - Fischer's exact test and 0.05 - Log rank test) [Figure 1]. Other complications like febrile neutropenia, mucositis,
renal dysfunction were also higher in children with folate deficiency but were not statistically significant.
Similarly, the transfusion requirements of folate deficient children were also higher as compared to
folate-sufficient children (packed red cell-2.6 ± 3.2 vs. 1.1 ± 1.8 units; P = 0.18, platelet concentrate 9.2 ± 20.2 vs. 3.0 ± 9.3 units; P = 0.36). Folate deficient children more often required a reduction in
the dose of Mtx in the subsequent cycles as compared to folate-sufficient children (40% vs. 9%; P = 0.14).
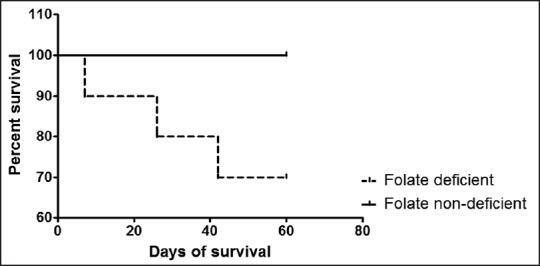
| Fig. 1 Survival in children receiving high-dose methotrexate according to their folate status
Though MTHFR 677 mutation was associated with an increased incidence of neutropenia, febrile neutropenia, mucositis, and hepatitis as compared to the wild genotype, none of these associations could reach statistical significance. Higher platelet transfusion requirement, longer chemotherapy interruption, and higher toxic deaths were also seen in 677 mutations but were not significant. Similar to the 677 genotypes, MTHFR 1298 mutations were also associated with higher incidence of neutropenia, mucositis, and hepatitis. They also had a higher transfusion requirements, longer chemotherapy interruptions, and greater need for dose-reduction in the subsequent cycles. However, of all these, the only significant association was with that of the requirement for packed red cell transfusion (3.4 ± 3.6 in 1298 mutations vs. 0.9 ± 1.6 units in 1298 wild genotype; P = 0.03).
DISCUSSION
This study investigated the impact of precourse folate deficiency and the MTHFR variants on chemotherapy toxicity and complications during HD-Mtx based therapy in children with ALL.
The pre-HD-Mtx folate levels in our patients did not correlate with the MTHFR genotypes. Though the levels were lower in children with MTHFR 677 and 1298 mutations they were not significantly different from those with the 677 and 1298 wild genotypes. The lack of significance may be due to the small number of patients who received HD-Mtx in our study. We could not find any other study on children with ALL where the folate levels were studied in relation to their MTHFR genotypes. One study assessing the precycle folate levels (serum and red cell) during HD-Mtx in children with osteosarcoma found a progressive increase in folate levels with increasing number of HD-Mtx cycles.[6] However, the clinical implications of these findings were not reported.
High dose methotrexate is known to cause a host of toxicities including hematological, hepatic, renal, gastrointestinal and mucocutaneous.[2,6] Mtx targets several critical steps in folate metabolism. Therefore it seems natural that serum folate levels at baseline would affect the pharmacobiology of HD-Mtx. However, studies assessing the effect of pretherapy folate status on the toxicities of HD-Mtx are limited.[6] Folate deficiency in children included in the present study was significantly associated with increased rate of complications including the incidence of neutropenia and a higher duration of interruption of chemotherapy. Our finding on increased incidence of neutropenia is supported by the study done on osteosarcoma patients which reported a lower nadir of leucocyte counts in patients who had precycle folate deficiency.[6] A previously published case report documented severe encephalopathy in a child on HD-Mtx for ALL and the encephalopathy occurred when the child was folate deficient prior to the Mtx dose, but it did not recur on the subsequent cycle prior to which the child's folate status was normalized,[7] none of our folate deficient children, however developed any central nervous system toxicity. Though other complications like febrile neutropenia, mucositis, need for Mtx dose reduction were also more common in the folate deficient children, they were not statistically significant. This lack of statistical significance might have been due to the inadequate sample size. Another study from the Czech Republic examining the pharmacokinetics of HD-Mtx, documented increasing folate levels with increasing number of HD-Mtx courses. They also observed higher peak Mtx levels in cycles with precycle folate deficiency but did not study the clinical implications.[8] Under ideal circumstances folate levels in our study should have been done prior to every dose of HD-Mtx to document dose to dose variation of folate status with higher doses of Mtx.[6] Moreover, we could not monitor the serum Mtx levels in our patients due to lack of resources.
Moreover, we did not find a single comparable study in literature which has reported the effect of folate deficiency on the complications encountered during HD-Mtx therapy for childhood ALL.
In stark contrast to the lack of studies on folate deficiency and toxicity of HD-Mtx, there have been a good number of studies in the literature which examined the association of MTHFR genotype with the complications of HD-Mtx.[8,9,10,11,12] Though this issue was investigated by various authors no consensus could be reached, and results have been mutually contradictory. The differences may have cropped in due to various reasons like sample size issues, non-uniform chemotherapy protocols including the dosage of Mtx and leucovorin. However, none of these studies included the folate status.
Mucositis, duration of chemotherapy interruption, transfusion requirements were higher in patients with MTHFR 677 (CT+TT) mutations, but none of them reached statistical significance probably due to low sample size. Though the lack of association of 677 mutation in our study compared favorably with some of the previous studies[13,14] many other studies have associated higher incidence of anemia, leukopenia, and thrombocytopenia with the presence of 677T allele.[9,11]
We did not observe any protective effect of MTHFR 1298 mutation as observed by few other studies,[13,14] our patients with 1298C allele had significantly higher requirement for red cell transfusion which corroborates with another study reporting higher incidence of anemia in children with 1298 mutations.[11] In our study group, higher incidence of neutropenia, mucositis, longer duration of chemotherapy intolerance was seen in children with 1298 mutations, though these were not statistically significant.
We also observed a higher incidence of toxic deaths during cycles of HD-Mtx in children who were folate deficient before the start of HD-Mtx. In fact, all the three patients who expired were folate deficient prior to therapy with HD-Mtx.
CONCLUSION
During HD-Mtx therapy, children with precourse folate deficiency had a higher incidence of neutropenia and longer duration of chemotherapy interruption as well as higher mortality. Children with 1298 mutations required higher number of units of red cell transfusion.
Financial support and sponsorship
Indian Council of Medical Research, New Delhi, India and Uttar Pradesh Council of Science and Technology, Lucknow, India.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
Indian Council of Medical Research, New Delhi, India and Uttar Pradesh Council of Science and Technology, Lucknow, India.
REFERENCES
| Fig. 1 Survival in children receiving high-dose methotrexate according to their folate status