 PDF
PDF  Views
Views  Share
Share


Embryonal rhabdomyosarcoma of the broad ligament
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2014; 35(01): 103-105
DOI: DOI: 10.4103/0971-5851.133734
Abstract
Broad ligament tumors are uncommon. Sarcomas rarely arise from the broad ligament, leiomyosarcomas being the most common. Rhabdomyosarcomas of the broad ligament are very rare. To the best of our knowledge, no case of an embryonal rhabdomyosarcoma of the broad ligament has been reported in literature.
Publication History
Article published online:
19 July 2021
© 2014. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Abstract
Broad ligament tumors are uncommon. Sarcomas rarely arise from the broad ligament, leiomyosarcomas being the most common. Rhabdomyosarcomas of the broad ligament are very rare. To the best of our knowledge, no case of an embryonal rhabdomyosarcoma of the broad ligament has been reported in literature.
INTRODUCTION
A study by Gardner et al. first described broad ligament tumors in 1957.[1] Leiomyosarcomas are the most common malignant broad ligament tumors.[2] Rhabdomyosarcomas arising from the broad ligament are very rare. We came across 3 cases of sarcomas, other than leiomyosarcomas, reported to arise from the broad ligament.[3,4,5] To the best of our knowledge, no case of an embryonal rhabdomyosarcoma (ERMS) of the broad ligament has been reported in literature. We report about a 9-month-old female child with an ERMS of the broad ligament.
The case we present here is a 9-month-old female child, presented to us with the complaints of straining at micturition and defecation since the age of 5 months. The patient was diagnosed with benign partial epilepsy of infancy and was under treatment for the same. No other comorbidities were present. On examination, the patient had multiple Café au lait spots over her body (more than 5 in number). However, there were no other features to suggest neurofibromatosis, like, family history, Lisch nodules, axillary or inguinal freckling and osseous lesions. Abdominal examination revealed an abdominopelvic mass, in the midline, extending superiorly to just above the umbilicus. The mass was firm to hard in consistency and mobile. The mass was also felt on per-rectal examination. A contrast enhanced computed tomography (CECT) scan of the abdomen and pelvis confirmed the clinical findings of an abdominopelvic mass of about 9.8 cm × 6 cm × 5 cm extending from the level of acetabulum in the pelvis, to the level of L3 vertebra [Figure 1]. The mass was isodense to hypodense on a plain scan with heterogenous enhancement on post-contrast scan. The urinary bladder was pushed to the right side due to mass effect but planes were maintained. There was mild left-sided hydronephrosis with the distal left ureter not visualized. The uterus and adnexa were not visualized separately. A percutaneous biopsy done from the mass revealed ERMS. The metastatic work-up, including a bone scan, CECT thorax and bone marrow examination, was normal.
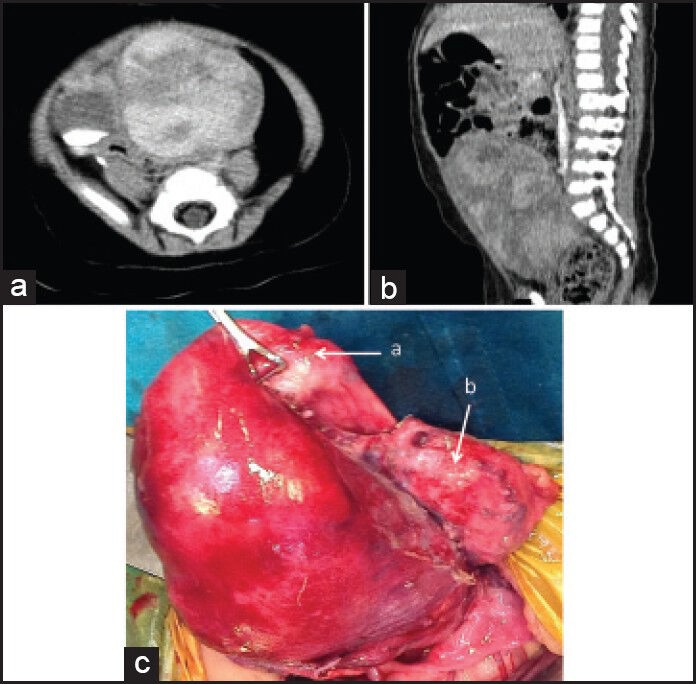
| Figure 1:Contrast enhanced computed tomography scan showing the heterogenously enhancing mass arising from pelvis, with contrast in urinary bladder (a and b). Intra-operatively (c), the mass seen arising from the broad ligament, the uterus (a) and urinary bladder (b) separated
The patient received neoadjuvant chemotherapy (NACT), as per intergroup rhabdomyosarcoma study group (IRS) IV protocol (vincristine, actinomycin and cyclophosphamide). The post NACT CECT scan showed a stable disease. An exploratory laparotomy performed revealed a lobulated mass of 10 cm × 5 cm × 5 cm [Figure 1]. The mass had a pedicle and was seen to be arising from the left broad ligament. The uterus and adnexa were separate from the mass, pushed to the right side. The mass was densely adhered to the urinary bladder but could be separated by dissection. The ureters on both sides were separate from the mass. The mass was excised in-toto preserving the uterus and the adnexae. The post-operative course of the patient was uneventful. The final histopathology revealed an ERMS with cut margin negative for tumor. The Immunohistochemistry studies were positive for desmin and myosin [Figure 2]. As per the TNM and IRS staging, our patient was staged as Stage I, Group III, with embryonal histology and thus classified as low risk subgroup.[6] The patient was treated with adjuvant chemotherapy as per IRS IV protocol.
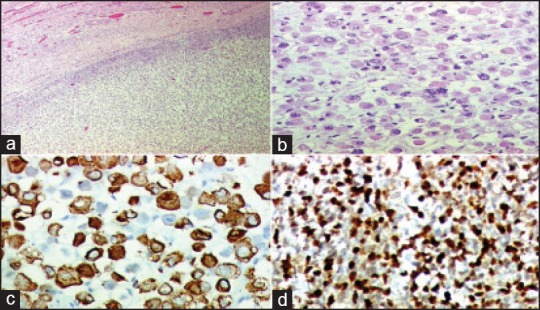
| Figure 2:Histology showing rhabdomyosarcomatous elements (a and b). Immunohistochemistry positive for desmin (c) and myosin (d)
DISCUSSION
Rhabdomyosarcoma is the most common soft-tissue sarcoma of children accounting for 3-4% of all the childhood cancers.[7] Pathologically, rhabdomyosarcoma is classified into three subtypes: Embryonal, alveolar and pleomorphic. ERMS forms 60% of the cases and is seen in younger patients. Sites commonly affected are head and neck and genitourinary systems. Rhabdomyosarcoma is known to be associated with Café au lait spots and neurofibromatosis type-I. Our patient though had Café au lait spots, did not have other features suggestive of neurofibromatosis.
On reviewing the literature on broad ligament sarcomas (excluding leiomyosarcomas), we came across only 3 such cases. Copeland et al. in their study have reported the first of those in 1985 in their series of eight patients of female genital tract sarcomas.[3] The patient was 16 years of age with an alveolar rhabdomyosarcoma of the broad ligament. The second case was a 55-year-old female diagnosed and treated for an undifferentiated pleomorphic sarcoma of the broad ligament reported by Bouraoui et al.[4] The third patient, reported by Diaz-Murillo et al. was a 27-year female with an undifferentiated round cell sarcoma of the broad ligament.[5] Our patient is a 9-month-old child with an ERMS of the broad ligament. All the three previously reported patients received multimodality treatment. The first two patients developed recurrence and did not survive beyond 1-year of diagnosis. The patient reported by Diaz-Murillo was followed-up for 12 years without any recurrence. Our patient is still receiving her adjuvant chemotherapy.
The treatment of rhabdomyosarcoma requires a multimodality approach. The treatment is decided after a tissue diagnosis and metastatic work-up of the patient. Our patient after appropriate investigations was diagnosed as a non-metastatic pelvic ERMS. On the basis of CECT scan findings of an abutting urinary bladder and non-visualization of the left ureter, it was decided to start NACT (IRS IV protocol)[8] and reassess for the response. On repeating a CECT scan after NACT, it was a stable disease; hence, it was decided to go ahead with surgery for appropriate local control of the tumor. A gross total excision of the tumor could be achieved. Adjuvant radiation therapy was considered in view of the mass adherent to the urinary bladder, but withheld considering the age and low risk group of the patient. Adjuvant chemotherapy was given.
CONCLUSION
Broad ligament rhabdomyosarcomas are an extremely rare entity. To the best of our knowledge, this is the first case of an ERMS arising from the broad ligament in an infant.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- Gardner GH, Greene RR, Peckham B. Tumors of the broad ligament. Am J Obstet Gynecol 1957;73:536-54.
- Chmaj-Wierzchowska K, Buks J, Wierzchowski M, Szymanowski K, Opala T. Leiomyoma cellulare in the broad ligament of the uterus - Case report and review of literature. Ginekol Pol 2012;83:301-4.
- Copeland LJ, Sneige N, Stringer CA, Gershenson DM, Saul PB, Kavanagh JJ. Alveolar rhabdomyosarcoma of the female genitalia. Cancer 1985;56:849-55.
- Bouraoui S, Mlika M, Blel A, Kamoun H, Mzabi-Regaya S. Undifferentiated pleomorphic sarcoma of the broad ligament. Pathologica 2008;100:478-81.
- Diaz-Murillo R, Iglesias-Sanchez C, Zapardiel I. Undifferentiated round cell sarcoma of the broad ligament. Ecancermedicalscience 2013;7:303.
- Malempati S, Hawkins DS. Rhabdomyosarcoma: Review of the children′s oncology group (COG) soft-tissue sarcoma committee experience and rationale for current COG studies. Pediatr Blood Cancer 2012;59:5-10.
- Wang LL, Yustein J, Louis T, Russell HV, Pappo AS, Paulino A et al. Solid tumors of childhood. In: Pine JW, editor. Hellman and Rosenberg′s Cancer Principles and Practice of Oncology. 9 th ed. Philadelphia: Lippincott Williams and Wilkins; 2011. p. 1760-92.
- Wu HY, Snyder HM 3 rd , Womer RB. Genitourinary rhabdomyosarcoma: Which treatment, how much, and when? J Pediatr Urol 2009;5:501-6.
| Figure 1:Contrast enhanced computed tomography scan showing the heterogenously enhancing mass arising from pelvis, with contrast in urinary bladder (a and b). Intra-operatively (c), the mass seen arising from the broad ligament, the uterus (a) and urinary bladder (b) separated
| Figure 2:Histology showing rhabdomyosarcomatous elements (a and b). Immunohistochemistry positive for desmin (c) and myosin (d)
References
- Gardner GH, Greene RR, Peckham B. Tumors of the broad ligament. Am J Obstet Gynecol 1957;73:536-54.
- Chmaj-Wierzchowska K, Buks J, Wierzchowski M, Szymanowski K, Opala T. Leiomyoma cellulare in the broad ligament of the uterus - Case report and review of literature. Ginekol Pol 2012;83:301-4.
- Copeland LJ, Sneige N, Stringer CA, Gershenson DM, Saul PB, Kavanagh JJ. Alveolar rhabdomyosarcoma of the female genitalia. Cancer 1985;56:849-55.
- Bouraoui S, Mlika M, Blel A, Kamoun H, Mzabi-Regaya S. Undifferentiated pleomorphic sarcoma of the broad ligament. Pathologica 2008;100:478-81.
- Diaz-Murillo R, Iglesias-Sanchez C, Zapardiel I. Undifferentiated round cell sarcoma of the broad ligament. Ecancermedicalscience 2013;7:303.
- Malempati S, Hawkins DS. Rhabdomyosarcoma: Review of the children′s oncology group (COG) soft-tissue sarcoma committee experience and rationale for current COG studies. Pediatr Blood Cancer 2012;59:5-10.
- Wang LL, Yustein J, Louis T, Russell HV, Pappo AS, Paulino A et al. Solid tumors of childhood. In: Pine JW, editor. Hellman and Rosenberg′s Cancer Principles and Practice of Oncology. 9 th ed. Philadelphia: Lippincott Williams and Wilkins; 2011. p. 1760-92.
- Wu HY, Snyder HM 3 rd , Womer RB. Genitourinary rhabdomyosarcoma: Which treatment, how much, and when? J Pediatr Urol 2009;5:501-6.