 PDF
PDF  Views
Views  Share
Share


Epidemiological review of laryngeal cancer: An Indian perspective
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2015; 36(03): 154-160
DOI: DOI: 10.4103/0971-5851.166721
Abstract
Background: Laryngeal cancer is one of the 10 leading causes of cancer in Indian men. The association of laryngeal cancer and tobacco smoking is well-established, but the peculiarities such as wide variation of disease distribution and survival, role of tobacco chewing, indoor air pollution, and dietary factors in laryngeal cancer causation needs to be understood. In this study, we review the descriptive and observational epidemiology of laryngeal cancer in India. Materials and Methods: MEDLINE and Web of science electronic database was searched from January 1995 to December 2013, using the using keywords "laryngeal cancer, laryngeal cancer outcome, epidemiology, etiological factor and their corresponding Mesh terms were used in combination like OR, AND." Two authors independently selected studies published in English and conducted in India. A total of 15 studies were found to be relevant and eligible for this review. Results: In India, laryngeal cancer contributes to approximately 3-6% of all cancers in men. The age-adjusted incidence rate of cancer larynx in males varies widely among registries, highest is 8.18 per 100,000 in Kamprup Urban District and the lowest is 1.26 per 100,000 in Nagaland. The 5-year survival for laryngeal cancer in India is approximately 28%. Indian studies show tobacco, alcohol, long-term exposure to indoor air pollution, spicy food, and nonvegetarian diet as risk factors for laryngeal cancer. Conclusion: There is wide regional variation in the incidence of laryngeal cancer in India. Survival rates of laryngeal carcinoma are much lower as compared to other Asian countries. Studies conducted in India to identify important risk factors of laryngeal cancer are very limited, especially on diet and indoor air pollution. Hence, more research is required for identifying the etiological factors and development of scientifically sound laryngeal cancer prevention programs.
Publication History
Article published online:
12 July 2021
© 2015. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Abstract
Background:
Laryngeal cancer is one of the 10 leading causes of cancer in Indian men. The association of laryngeal cancer and tobacco smoking is well-established, but the peculiarities such as wide variation of disease distribution and survival, role of tobacco chewing, indoor air pollution, and dietary factors in laryngeal cancer causation needs to be understood. In this study, we review the descriptive and observational epidemiology of laryngeal cancer in India.
Materials and Methods:
MEDLINE and Web of science electronic database was searched from January 1995 to December 2013, using the using keywords “laryngeal cancer, laryngeal cancer outcome, epidemiology, etiological factor and their corresponding Mesh terms were used in combination like OR, AND.” Two authors independently selected studies published in English and conducted in India. A total of 15 studies were found to be relevant and eligible for this review.
Results:
In India, laryngeal cancer contributes to approximately 3-6% of all cancers in men. The age-adjusted incidence rate of cancer larynx in males varies widely among registries, highest is 8.18 per 100,000 in Kamprup Urban District and the lowest is 1.26 per 100,000 in Nagaland. The 5-year survival for laryngeal cancer in India is approximately 28%. Indian studies show tobacco, alcohol, long-term exposure to indoor air pollution, spicy food, and nonvegetarian diet as risk factors for laryngeal cancer.
Conclusion:
There is wide regional variation in the incidence of laryngeal cancer in India. Survival rates of laryngeal carcinoma are much lower as compared to other Asian countries. Studies conducted in India to identify important risk factors of laryngeal cancer are very limited, especially on diet and indoor air pollution. Hence, more research is required for identifying the etiological factors and development of scientifically sound laryngeal cancer prevention programs.
INTRODUCTION
Laryngeal cancer is the ninth and seventh most common cause of cancer in males in Asia and India respectively. In 2012, an estimated 25,446 new case were diagnosed, and 17,560 Indians lost their lives from laryngeal cancer.[1] In India, the incidence of laryngeal cancer has been reported to be 1.26-8.18 per 100,000 population, in different regions in the country.[2] Epidemiological studies carried out on laryngeal cancer have highlighted the peculiarities of the disease, like varying risk factors and wide regional variation in incidence and survival. This review includes an update on the distribution of laryngeal cancer in India, as well as publication on the association between various risk factors.
MATERIALS AND METHODS
Data sources and searches
Information was gathered from a review of peer-reviewed publications on laryngeal cancer in India. MEDLINE (http://www.pubmed.com) and Web of science electronic database was searched from January 1995 to December 2013, using the using keywords such as “laryngeal cancer, treatment, clinical characteristics, laryngeal cancer outcome, epidemiology, etiological factor and their corresponding Mesh terms were used in combination like OR, AND.” We also examined bibliographies of included articles to identify additional references. The search strategy was limited to English language. Only journal article type was included. Figure 1 presents the search strategy and screening process.
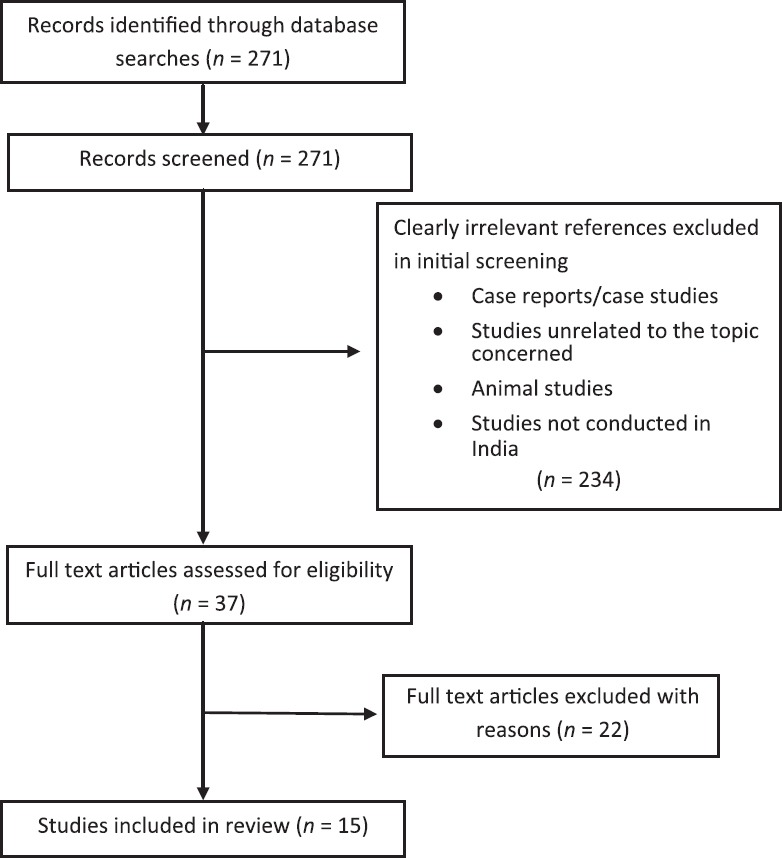
| Fig. 1 Summary of evidence search and selection
Study selection
Inclusion criteria
- Study designs eligible for inclusion in our review were randomized controlled trials, nonrandomized controlled trails, cohort studies and cross-sectional studies conducted to assess the disease distribution, its risk factors, survival, and any other factors affecting epidemiology of laryngeal cancer.
- Studies conducted in India only were included in the review.
Exclusion criteria
- Studies not conducted in India were excluded from the review.
Data extraction and analysis
The title and abstract of each citation were screened first, and full report was screened next, if necessary, to select the relevant articles according to selection the criteria. Full texts of these selected studies were retrieved, reviewed and extracted for relevant data by authors independently. A total of 15 studies were included in the review and their findings presented. The descriptive statistical data for laryngeal cancer were mainly obtained from publications of the Indian Cancer Registry, UICC, International Agency for Research on Cancer (IARC) and WHO (GLOBOCON-2012).
Descriptive epidemiology
The Indian cancer registries include 25 Population Based Cancer Registries (PBCR) and 07 Hospital Based Cancer Registries (HBCR), of the 25 PBCR's, 11 PBCR's are urban, 02 are rural and remaining 12 correspond to urban and rural both by virtue of being state or district registries.[2] The data obtained from these Indian Cancer Registries indicates that in India cancer larynx is far more common in males as compared to females. Laryngeal cancer contributes to approximately 3-6% of all cancer in males and only about 0.2-1% of all cancers in females.[2] The age-adjusted incidence rate of cancer larynx in males was found to vary widely among registries, highest being 8.18 per 100,000 in Kamprup Urban District and the lowest being 1.26 per 100,000 in Nagaland followed by 1.55 per 100,000 in Barshi rural. Most of the registries in western and central India have an age-adjusted incidence rate of cancer larynx between 3.5 and 5 per 100,000 population. However, certain older, cancer registries such as Delhi and Bhopal have reported a higher age-adjusted incidence rate of 7.61 and 6.43 per 100,000 respectively[2] [Table 1]. This wide variation of age-adjusted incidence rate among registries need to be interpreted cautiously as many registries are newly established and it has been demonstrated that in their initial years of operation, registries might include prevalent cases or may also miss certain cases till they are well established. Similar to global trends of cancer larynx, Delhi and Mumbai registries have also shown a statistically significant decreasing trend over the past 25 years. However, the Bhopal registry reported a statistically significant increasing trend of cancer larynx[3] [Table 2].
Table 1
Age-adjusted (world) incidence and mortality rates of larynx cancer* and its relative proportion in Indian PBCR
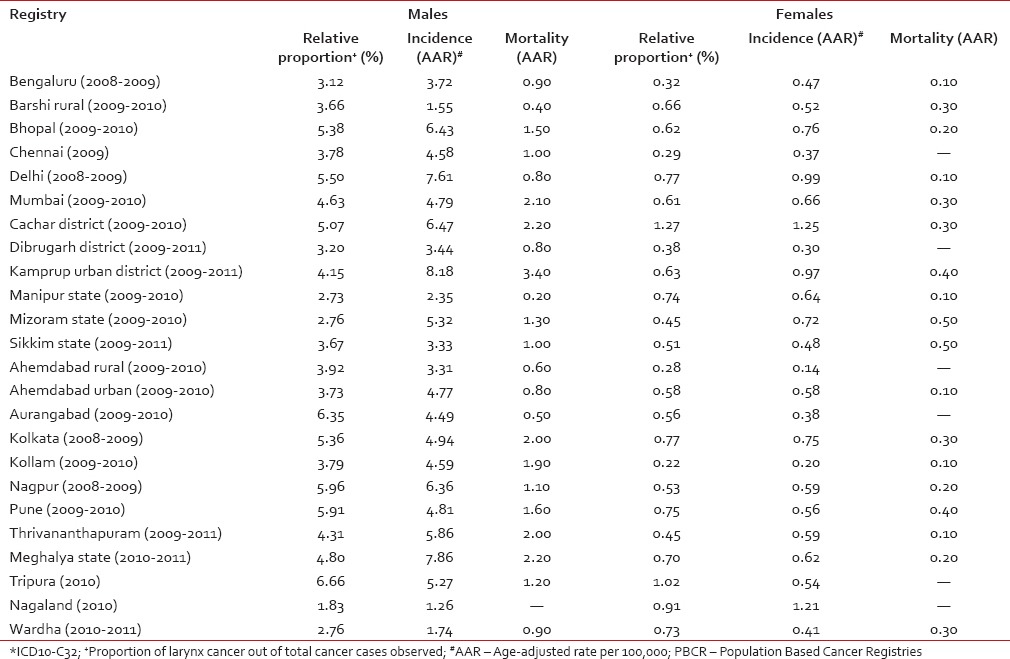
Table 2
The age-adjusted (world) incidence rates and APC for larynx cancer in males in Indian PBCR during the years 1982-2009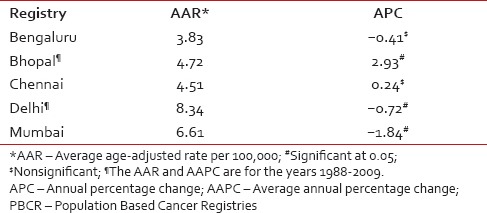
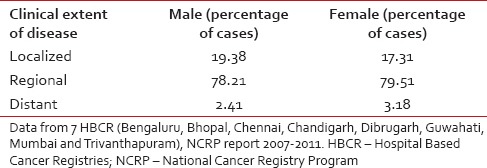
More than 50% of patients in both males and females were older than 60 years. The maximum numbers of cases were reported in the age group of 60-69 years amounting to 31.93% of all larynx carcinoma in males and 27.29% in females[2] [Table 3]. Data from HBCR show that almost 70% of all female cases and 50% of male cases were either illiterate or had primary level education[4] [Table 4]. Data from HBCR also indicate that almost 80% of both male and female cases had regional diseases at the time of presentation[5] [Table 5].
Table 3
Age-wise distribution of larynx cancer
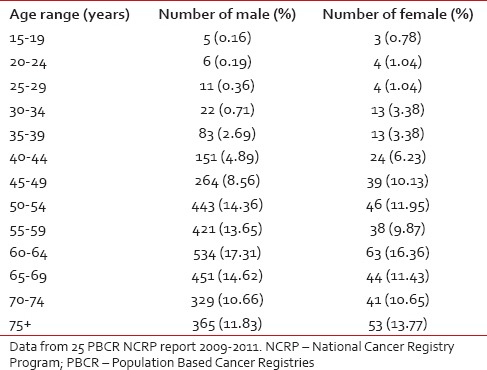
Table 4
Distribution of larynx cancer as per educational status
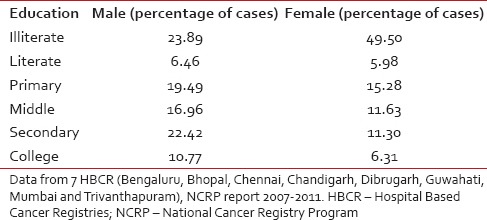
Table 5
Clinical extent of the disease (larynx cancer) at presentation
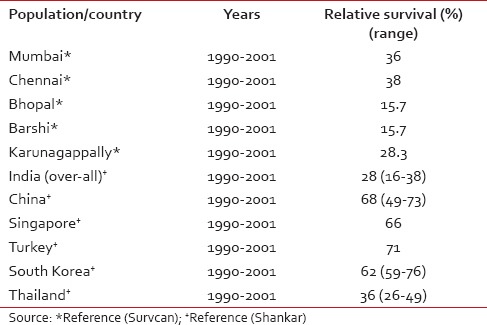
The 5-year survival rate for cancer larynx in India is approximately 28%.[6] This indicates that prognosis from cancer larynx remains poor as compared to other Asian countries such as China, South Korea, and Singapore [Table 6]. A wide variation of survival rates is also observed between rural and urban India. This could be because Indian registries suffer with the problem of under-reporting of death, which is more pronounced in the rural area. In addition, the lack of health infrastructure in rural India results in lower survival rates as compared to urban areas. The 5-year age-standardized relative survival of laryngeal cancer for different Indian registries and its comparison with other Asian registries is shown in Table 6.[6,7]
Table 6
5-year age standardized (0-74 years) relative survival for laryngeal cancer in selected Indian populations and selected Asian countries
Risk factors
Tobacco
The most important risk factor for cancer larynx appears to be the tobacco use. National Cancer Registry Program enlists laryngeal cancer as one of the tobacco-related cancer.[8] The IARC monograph also classifies tobacco use as a carcinogenic to humans based on overwhelming on epidemiological evidence.[9] A large number of case-control and cohort studies conducted in various parts of the world have observed many fold increase in cancer larynx with the use of various forms of tobacco.[10,11,12]
In India, tobacco is both chewed and smoked in several forms. A common form of smoking tobacco is “bidi” an Indian cigarette, containing 0.2-0.3 g of tobacco rolled in a dried leaf, usually temburni leaf (Diospyros mylanoxylon). The other types of smoking in India are described by Sanghvi et al.[13] Many studies on laryngeal cancer in India implicated smoking as a risk factor. The risk level varied from 1.5-fold to 7-fold for different forms of tobacco smoking. In one of the earlier studies, Rao et al.[14] found that biddi and cigarette smoking to be associated with cancer of the larynx, however, the risk of laryngeal cancer was found to be much more for bidi than for cigarette. Other subsequent case-control studies also found bidi and cigarette smoking to be significantly associated with laryngeal carcinoma.[15,16,17] A cohort study of 65,553 men aged 30-84 in Karunagappally Taluk, Kerala also found that laryngeal cancer was strongly related to bidi and cigarette smoking as well as the number smoked per day (P < 0.001) and duration of smoking (P < 0.001), bidi smoking was found to have higher risk than cigarette smoking [Table 7].[18]
Table 7
Association between tobacco and carcinoma larynx
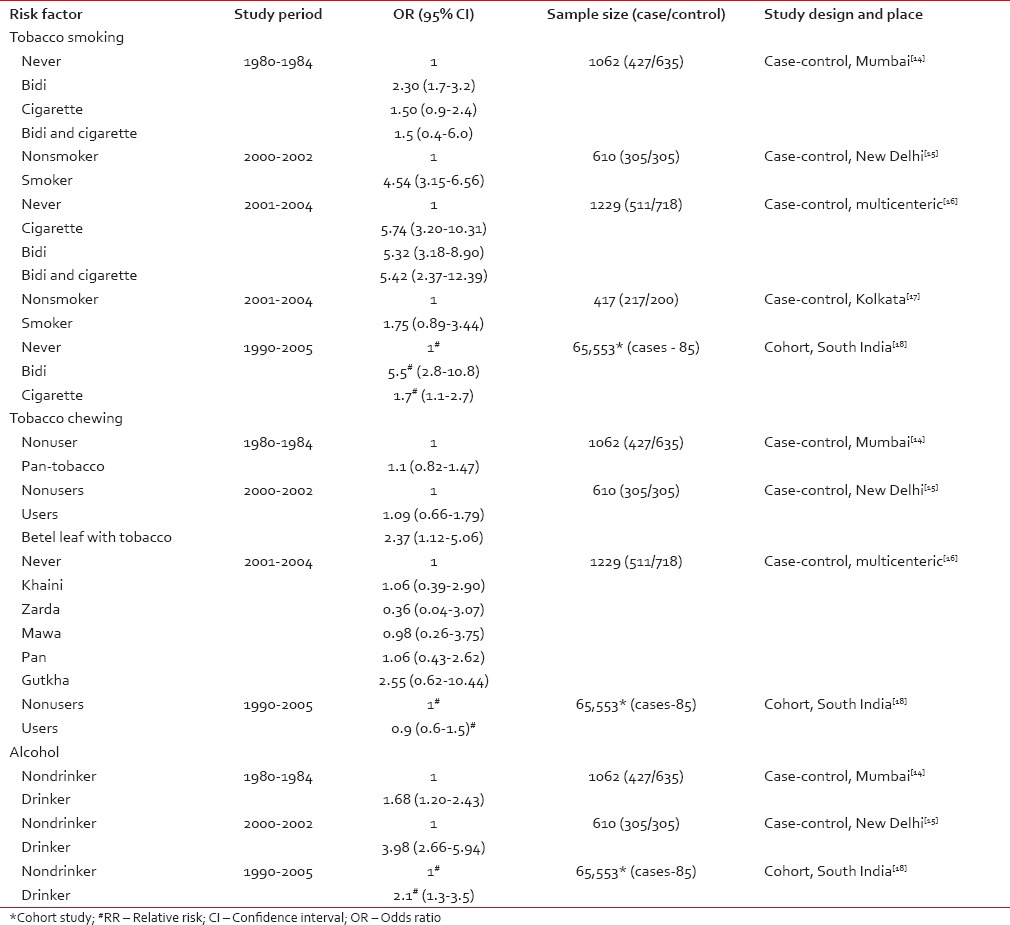 Chewing of tobacco in the form of khaini, zarda, mawa, pan, etc. is also prevalent in India. Many studies including a large multicentric case-control study of 511 laryngeal cancer cases have not found tobacco chewing as a risk factor for laryngeal carcinoma.[14,15,16,18,19] However, Kapil et al. in a hospital-based case-control study consisting of 305 laryngeal cancer patients found chewing of betel leaf with tobacco to increase the risk for laryngeal cancer by 2.37-fold but like other studies it failed to find any association between cancer larynx and tobacco chewing.
Chewing of tobacco in the form of khaini, zarda, mawa, pan, etc. is also prevalent in India. Many studies including a large multicentric case-control study of 511 laryngeal cancer cases have not found tobacco chewing as a risk factor for laryngeal carcinoma.[14,15,16,18,19] However, Kapil et al. in a hospital-based case-control study consisting of 305 laryngeal cancer patients found chewing of betel leaf with tobacco to increase the risk for laryngeal cancer by 2.37-fold but like other studies it failed to find any association between cancer larynx and tobacco chewing.Alcohol
Besides tobacco use, alcohol consumption has also been implicated as a risk factor in the development of laryngeal carcinoma. There is a dearth of Indian studies on the association between alcohol and laryngeal cancer, mainly due to social stigma associated with the alcohol habit and ban on alcohol drinking in certain states of India. Furthermore, women in India do not openly admit to the habit of alcohol consumption.[14] However, a few case-control studies and one cohort study found an almost 2-4-fold increase in risk of laryngeal cancer due to alcohol consumption [Table 7].[14,15,16] These studies, provide evidence of alcohol as an additional risk factor for laryngeal carcinoma, which is in conformity with several western studies.[10,11,12,20,21]
Indoor air pollution
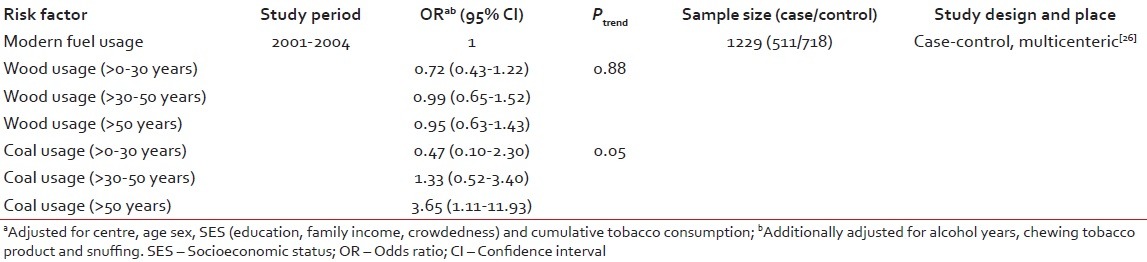
Table 8
Association between indoor air pollution and carcinoma larynx (OR by type and duration of fuel usage)
Dietary factors
Data on the nutritional factors associated with cancer of the larynx is limited. A hospital-based case-control study consisting of 305 laryngeal cancer patients conducted during 2000-2002, assessed the role of dietary items such as fruits, vegetables, egg, meat, and spicy food.[15] The study reported that there was an inverse association between the risk of laryngeal cancer and consumption of roots and tubers, vegetables, and fruits. The risk of laryngeal cancer was found to be 5.25, 5.67, and 3.28 times higher for those who consumed roots and tubers, green leafy vegetables and fruits < 4 times per week.[15] A 2-3-fold increase in risk of laryngeal cancer was also observed with consumption of eggs, meat, and spicy food. However, Rao et al. in his case-control study of 427 subjects failed to find any association between nonvegetarian diet and laryngeal cancer.[14] An earlier study (Notani and Jayant, 1987) reported the similar inverse relationship between laryngeal cancer and consumption of fruit and vegetables.[27] Several Western studies also reported reduced laryngeal cancer risk with consumption of fruits and vegetables.[28,29,30] The studies on diet and laryngeal cancer though few, provide a window of opportunity to study further the role of vegetarian diet in the prevention of laryngeal cancer.
Prevention
It is very evident from the large number of studies conducted across the globe that tobacco and alcohol are perhaps important risk factors for laryngeal cancer. The risk rises with increasing levels of smoking and alcohol drinking, each agent approximately multiplying the effects of the other.[31,32] Thus, studies conducted to examine the effect of stopping smoking, drinking or both have demonstrated that the risk laryngeal cancer appears to decline steeply with time, by over 70% in 10 or more years after stopping smoking,[33,34,35] however the similar clear pattern with stoppage of drinking has not been demonstrated.[35,36,37] These effects of smoking and drinking cessation are from western studies, and similar studies have not been done in India. Indians have one of the most interesting diets, with many unique dietary constituents that have promise for cancer prevention. A few epidemiological studies exploring the relationships between diet, lifestyle and cancer have been carried out in India, but none in respect of diet and prevention of laryngeal carcinoma.
Opinions are divided about screening for cancer in the early stage and for hyperplastic alterations of the laryngeal mucosa. No screening trails for laryngeal cancer have been conducted in India. The few trails conducted in western population considering availability, the time and effort required for the conduct of screening test, have not recommended screening for laryngeal cancer.[38]
CONCLUSIONS
Laryngeal cancer has a varying distribution in India. Some regions report a decreasing while others report an increasing trend. Indian studies have well-established tobacco smoking and alcohol as major risk factors for laryngeal carcinoma. Studies from India exploring the role of factors such as diet and indoor air pollution are limited. There is a need to conduct well-designed studies to understand the etiology of laryngeal cancer and implement preventive programs.
Financial support and sponsorship
Nil.
Conflicts of interest
REFERENCES
| Fig. 1 Summary of evidence search and selection