 PDF
PDF  Views
Views  Share
Share


Extraskeletal osteosarcoma: An uncommon variant with rare metastatic sites detected with FDG PET/CT
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2014; 35(01): 96-98
DOI: DOI: 10.4103/0971-5851.133732
Abstract
Extraskeletal osteosarcoma (ESOS) is a rare malignancy, which commonly presents with metastatic disease. Like their osteogenic counterparts, these tumors commonly metastasize to lungs and bones. We report the fluoro-deoxyglucose positron emission tomography findings in a case of ESOS presenting with a combination of rare metastatic sites such as brain, kidney and the bone marrow.
Publication History
Article published online:
19 July 2021
© 2014. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Abstract
Extraskeletal osteosarcoma (ESOS) is a rare malignancy, which commonly presents with metastatic disease. Like their osteogenic counterparts, these tumors commonly metastasize to lungs and bones. We report the fluoro-deoxyglucose positron emission tomography findings in a case of ESOS presenting with a combination of rare metastatic sites such as brain, kidney and the bone marrow.
INTRODUCTION
Extraskeletal osteosarcoma (ESOS) is a rare aggressive tumor, which commonly presents with disseminated metastases.[1] Lungs and bones are common sites of metastatic involvement in osteosarcoma at initial presentation as well as after completion of treatment. Computed tomography (CT) scan of the chest and bone scan are routinely used to detect lung and bone metastases in osteogenic sarcomas.[2] With the advent of 18F-fluoro-deoxyglucose (18F-FDG) positron emission tomography/computed tomography (PET/CT) imaging, unusual and often rare sites of metastatic spread have been uncovered in several malignancies. In this report, we describe an extremely rare combination of unusual metastatic sites from ESOS on FDG PET/CT.
A 32-year-old female patient presented to our Institution with a bulky left supraclavicular mass. The swelling was noticed 3 months back and had rapidly grown in size over the past month, with no accompanying pain. On examination, a hard, non-tender, mobile mass was felt in the left supraclavicular fossa, separate from the adjacent bones, in a relaxed posture, which became taut on shrugging or moving left shoulder. A biopsy specimen from the mass, on histopathological examination revealed osteoid deposition by tumor cells, with osteoclastic giant cells and pleomorphic malignant cells within the osteoid, suggestive of osteosarcoma [Figure 1]. Thus, correlation of clinical, imaging and histopathological findings confirmed the diagnosis of ESOS. Patient was then referred for a whole body 18F-FDG PET/CT study for pre-treatment staging. Maximum Intensity Projection (MIP) images [Figure 2a] revealed a large focus of tracer concentration in left supraclavicular region [Figure 2a arrow], with multiple foci of uptake in the right hemithorax, region of the right kidney, left pelvis, mid thorax and abdomen [Figure 2a all arrowheads]. Fused axial PET/CT images showed tracer uptake in a bulky soft-tissue mass arising from the left trapezius muscle, [Figure 2b arrow], which was the site of primary malignancy. There was no involvement of left scapula noted on the CT component of the study, confirmed on coronal oblique CT [Figure 2c arrow] and PET/CT [Figure 2d arrow] images. Furthermore seen was intense FDG uptake in the right lung mass, left iliac bone marrow [Figure 3b arrow], D12 vertebra [Figure 3c arrow], within a soft-tissue deposit in the left internal oblique muscle [Figure 3d arrow], in right renal cortex [Figure 3e arrow] and in medial end of left clavicle. Also noted was tracer uptake in the brain, which correlated to a soft-tissue lesion in right paraventricular region, with specks of calcification within, seen on axial fused PET/CT [Figure 3a arrow]. Thus, in addition to the common sites of metastases in the lungs and bones, FDG PET/CT detected metastatic deposits at unusual sites such as brain, renal parenchyma, marrow and skeletal muscle.
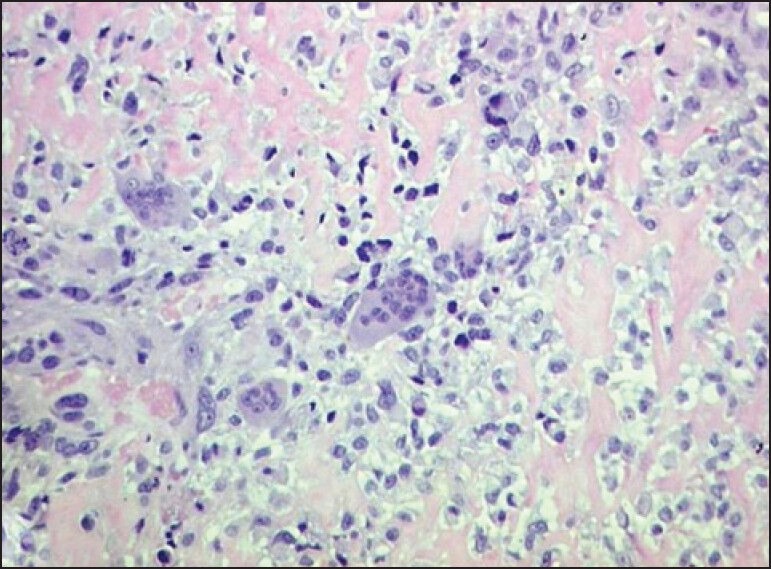
| Figure 1:Photomicrograph of pathology section showing osteoclastic giant cells and pleomorphic malignant cells amidst osteoid (H and E, × 200)
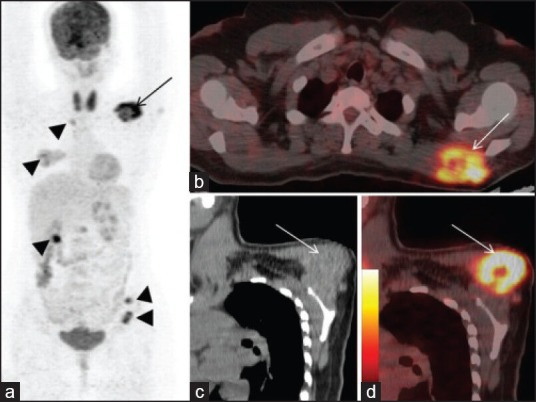
| Figure 2:(a) Maximum intensity projection image showing tracer uptake in left supraclavicular region (2a-arrow), in the region of mid thorax, mid abdomen, right lung, right kidney, left pelvis (all arrow heads) (b) axial fused PET/CT images show FDG avid mass arising from left trapezius muscle (arrow) (c) oblique coronal CT and fused PET/CT (d) images show origin of the mass from left trapezius, with no involvement of left scapula
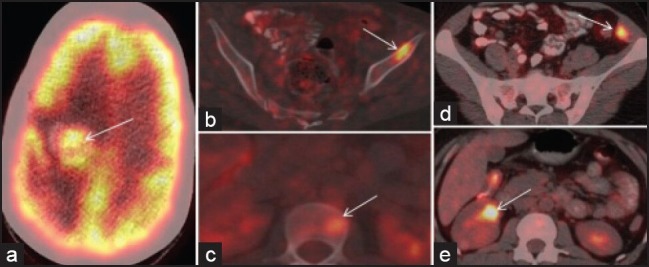
| Figure 3:Axial fused PET/CT images show FDG avid metastatic lesions in brain (a – arrow), left iliac marrow (b – arrow), D12 vertebral body (c – arrow), left internal oblique muscle (d – arrow) and right renal cortex (e – arrow)
DISCUSSION
ESOS is a rare tumor, accounting for 1% of all soft-tissue sarcomas and 4% of osteogenic osteosarcomas.[1,2] Though it is histologically similar to osteogenic osteosarcoma, it is demographically, clinically and therapeutically different from it.[3] It most commonly presents as a rapidly growing soft-tissue mass, either with or without pain; with lower extremity being the most common site and thigh accounting for 48% of the lesions, followed by upper extremity (8-23%), retroperitoneum (8-17%) and trunk (10-11%).[4] Metastatic spread is common, with many patients of ESOS presenting with metastatic disease. Lung is the most common site of metastases (80-88%), similar to osteogenic osteosarcoma; other metastatic sites being soft-tissue, bone (8-19%), liver (8-17%), peritoneum and adrenal glands (<5 href="https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4080674/#ref4" rid="ref4" class=" bibr popnode tag_hotlink tag_tooltip" id="__tag_387069129" role="button" aria-expanded="false" aria-haspopup="true" xss=removed>4,5] Since ESOS is generally a high grade spindle cell malignancy, the primary tumor as well as metastatic sites demonstrate FDG avidity. Fusion with CT helps to characterize the lesions, which show the presence of mineralized material within the soft-tissue and also provides an anatomical dimension to the FDG uptake. The existing literature on FDG PET/CT in ESOS confirms the fact that these tumors are FDG avid,[6,7] however all these reports demonstrate a single metastatic site, unlike multiple and rare sites demonstrated in our report. A single report also shows a tumor thrombus detected on FDG PET/CT.[7] Metastases to the kidney have not been reported so far in the existing literature. Metastases to the brain are extremely rare, with only a single case detected on histopathology, after surgical resection was performed in 21 patients with intraparenchymal brain metastases from sarcoma.[8] Though bone involvement is commonly seen, discrete marrow metastases have not been reported yet. Thus, a whole body metabolic imaging modality like FDG PET/CT is the investigation of choice in such high grade rare malignancies, which are aggressive at presentation. It is very well-known that the management of metastatic disease is not altered based on the number of sites of distant metastases. FDG PET/CT detects rare metastatic sites, which are not only an interesting finding, but also a valuable addition to the existing literature on metastatic sites of ESOS. Such documentation is of value, for a rare subgroup of patients who can present with metastases, from an unknown primary site, wherein, ESOS can emerge as one of the likely primary.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- Allan CJ, Soule EH. Osteogenic sarcoma of the somatic soft tissues. Clinicopathologic study of 26 cases and review of literature. Cancer 1971;27:1121-33.
- Eftekhari F. Imaging assessment of osteosarcoma in childhood and adolescence: Diagnosis, staging, and evaluating response to chemotherapy. Cancer Treat Res 2009;152:33-62.
- Bane BL, Evans HL, Ro JY, Carrasco CH, Grignon DJ, Benjamin RS, et al. Extraskeletal osteosarcoma. A clinicopathologic review of 26 cases. Cancer 1990;65:2762-70.
- Lee JS, Fetsch JF, Wasdhal DA, Lee BP, Pritchard DJ, Nascimento AG. A review of 40 patients with extraskeletal osteosarcoma. Cancer 1995;76:2253-9.
- Chung EB, Enzinger FM. Extraskeletal osteosarcoma. Cancer 1987;60:1132-42.
- Mc Auley G, Jagannathan J, O′Regan K, Krajewski KM, Hornick JL, Butrynski J, et al. Extraskeletal osteosarcoma: Spectrum of imaging findings. AJR Am J Roentgenol 2012;198:W31-7.
- Tateishi U, Yamaguchi U, Terauchi T, Maeda T, Moriyama N, Arai Y, et al. Extraskeletal osteosarcoma: Extensive tumor thrombus on fused PET-CT images. Ann Nucl Med 2005;19:729-32.
- Bindal RK, Sawaya RE, Leavens ME, Taylor SH, Guinee VF. Sarcoma metastatic to the brain: Results of surgical treatment. Neurosurgery 1994;35:185-90.
| Figure 1:Photomicrograph of pathology section showing osteoclastic giant cells and pleomorphic malignant cells amidst osteoid (H and E, × 200)
| Figure 2:(a) Maximum intensity projection image showing tracer uptake in left supraclavicular region (2a-arrow), in the region of mid thorax, mid abdomen, right lung, right kidney, left pelvis (all arrow heads) (b) axial fused PET/CT images show FDG avid mass arising from left trapezius muscle (arrow) (c) oblique coronal CT and fused PET/CT (d) images show origin of the mass from left trapezius, with no involvement of left scapula
| Figure 3:Axial fused PET/CT images show FDG avid metastatic lesions in brain (a – arrow), left iliac marrow (b – arrow), D12 vertebral body (c – arrow), left internal oblique muscle (d – arrow) and right renal cortex (e – arrow)
References
- Allan CJ, Soule EH. Osteogenic sarcoma of the somatic soft tissues. Clinicopathologic study of 26 cases and review of literature. Cancer 1971;27:1121-33.
- Eftekhari F. Imaging assessment of osteosarcoma in childhood and adolescence: Diagnosis, staging, and evaluating response to chemotherapy. Cancer Treat Res 2009;152:33-62.
- Bane BL, Evans HL, Ro JY, Carrasco CH, Grignon DJ, Benjamin RS, et al. Extraskeletal osteosarcoma. A clinicopathologic review of 26 cases. Cancer 1990;65:2762-70.
- Lee JS, Fetsch JF, Wasdhal DA, Lee BP, Pritchard DJ, Nascimento AG. A review of 40 patients with extraskeletal osteosarcoma. Cancer 1995;76:2253-9.
- Chung EB, Enzinger FM. Extraskeletal osteosarcoma. Cancer 1987;60:1132-42.
- Mc Auley G, Jagannathan J, O′Regan K, Krajewski KM, Hornick JL, Butrynski J, et al. Extraskeletal osteosarcoma: Spectrum of imaging findings. AJR Am J Roentgenol 2012;198:W31-7.
- Tateishi U, Yamaguchi U, Terauchi T, Maeda T, Moriyama N, Arai Y, et al. Extraskeletal osteosarcoma: Extensive tumor thrombus on fused PET-CT images. Ann Nucl Med 2005;19:729-32.
- Bindal RK, Sawaya RE, Leavens ME, Taylor SH, Guinee VF. Sarcoma metastatic to the brain: Results of surgical treatment. Neurosurgery 1994;35:185-90.