 PDF
PDF  Views
Views  Share
Share


Flagellate Rash: An Unusual Complication of Bleomycin Therapy – A Case Report with Brief Review of Literature
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2017; 38(04): 548-551
DOI: DOI: 10.4103/ijmpo.ijmpo_147_16
Abstract
Chemotherapy-induced skin rashes arecommon toxicities encountered which require careful assessment and evaluation as rashes could be a manifestation of primary malignancy itself and a variety of drugs used incombination furthercomplicate the clinical scenario. Bleomycin is an anticancer antibiotic derived from Streptomyces verticillus and has beencommonly used in the treatment of Hodgkin's disease, germ cell tumors and for pleurodesis. There are various dermatological adverse effects of bleomycin which have been previously reported in literature including skin peeling, hyperkeratosis, nail bed changes, Raynaud's phenomenon, and palmoplantar desquamation. Bleomycin-induced skin rashes are seen infrequently now a day due to its declining use in clinical practice. We report here a 29-year-old male with Stage III germ cell tumor who developed widespread flagellate rash after receiving 3 cycles of bleomycin-based chemotherapy which responded to treatment with local steroids and omission of bleomycin from further chemotherapy cycles.
Publication History
Article published online:
04 July 2021
© 2017. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used forcommercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Abstract
Chemotherapy-induced skin rashes are common toxicities encountered which require careful assessment and evaluation as rashes could be a manifestation of primary malignancy itself and a variety of drugs used in combination further complicate the clinical scenario. Bleomycin is an anticancer antibiotic derived from Streptomyces verticillus and has been commonly used in the treatment of Hodgkin's disease, germ cell tumors and for pleurodesis. There are various dermatological adverse effects of bleomycin which have been previously reported in literature including skin peeling, hyperkeratosis, nail bed changes, Raynaud's phenomenon, and palmoplantar desquamation. Bleomycin-induced skin rashes are seen infrequently now a day due to its declining use in clinical practice. We report here a 29-year-old male with Stage III germ cell tumor who developed widespread flagellate rash after receiving 3 cycles of bleomycin-based chemotherapy which responded to treatment with local steroids and omission of bleomycin from further chemotherapy cycles.
Bleomycin is an antitumor antibiotic which was discovered in 1966 by Umezewa.[1] It exerts its cytotoxic effects by the generation of oxygen free radicals causing single and double stranded DNA breaks and eventual cell death. There is declining use of bleomycin in current practice due to its toxicity concerns; however, it is still widely used in Hodgkin's disease, germ cell tumors and for pleurodesis. It is inactivated by a cytosolic cysteine proteinase enzyme bleomycin hydrolase which is widely distributed in normal tissues with the exception of the skin and lungs, both targets of bleomycin toxicity.[2] Systemic elimination of the drug by enzymatic degradation is probably only important in patients with severely compromised renal function.
Skin reactions are the most common side effects and are relatively late manifestation usually developing after several cycles of chemotherapy has been administered and when the cumulative dose has reached 150–200 U, although it can occur with any dose of bleomycin.[1] Various dermatological adverse effects of bleomycin have been reported in the literature which includes skin peeling, hyperkeratosis, nail bed changes, Raynaud's phenomenon, and palmoplantar desquamation.[2] An unusual “Whip-like” linear streak rash which is described as “Flagellate rash” has also been reported to occur as a side effect of bleomycin therapy. The term “Flagellate” is derived from latin word “flagellum” referring to characteristic whip-like the appearance of the eruption. It occurs in 10% of patients treated with Bleomycin.[3]
We herein report a 29-year-old patient, who was on bleomycin-based chemotherapy for Stage III germ cell tumor, developed a widespread flagellate rash after receiving 3 cycles of bleomycin which responded to treatment with local steroids and omission of the drug from further chemotherapy cycles.
A 29-year-old male patient, with no prior known medical or dermatological comorbidities or any drug allergy, was diagnosed as a case of Stage IIIB testicular cancer. Contrast-enhanced computed tomography chest, and abdomen was suggestive of the lobulated lesion in paraaortic region with multiple bilateral lung nodules, mediastinal, and hilar lymphadenopathy [Figure 1]. Preoperative tumor marker analysis revealed serum alpha-feto protein level 12,100 ng/ml, serum beta human chorionic gonadotropin (HCG) level 2.39 mIU/ml, and serum lactate dehydrogenase (LDH) level 819 U/L. He underwent right high inguinal orchiectomy in May 2015. Final histopathology report was suggestive of mature cyctic teratoma of right testis with associated features of intratubular germ cell neoplasia [Figure 2]. Postoperative tumor marker analysis revealed serum alpha-feto protein level 126 ng/ml, serum beta-HCG level 2.39 mIU/ml and serum LDH level 292 U/L. Patients pulmonary and renal function tests were normal. He was started on bleomycin (30 units on days 1, 8, and15), etoposide (100 mg/m2 on day 1–5), and cisplatin (20 mg/m2 on day 1–5) based chemotherapy (BEP chemotherapy) as per our institutional protocol. However, after 3 cycles of chemotherapy, the patient started complaining of pruritic linear rashes which patient noticed first over the trunk and then gradually increased to involved skin over the chest, back, shoulder, and bilateral upper and lower limbs [Figure 3]. On physical examination, linear and streaked pigmentation were seen on bilateral upper limbs, lower limbs, and over chest and back. No other skin lesions were noted. There was no mucosal involvement or systemic upset. A clinical diagnosis of bleomycin-induced flagellate rash and postinflammatory pigmentation was considered. Routine laboratory investigations, including liver and renal function tests, were normal. Bleomycin was withheld from subsequent chemotherapy cycles, and the patient was prescribed betamethasone dipropionate ointment for local application twice a day for 2 weeks. On subsequent follow ups, the itching sensation was reduced was mild hyperpigmentation remained [Figure 4].
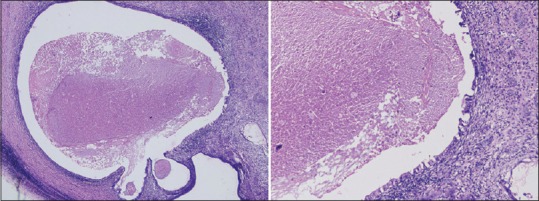
| Figure 1:Histopathology slides showing mature cystic teratoma with Intratubular germ cell neoplasia
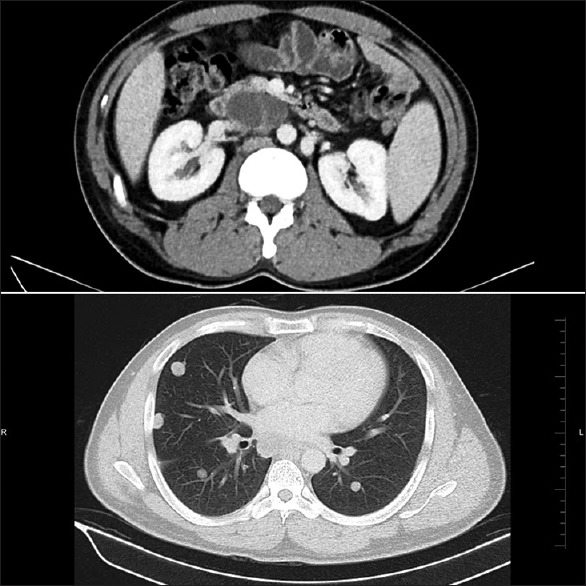
| Figure 2:Contrast-enhanced computed tomography abdomen chest showing multiple bilateral lung nodules with mediastinal and hilar lymphadenopathy

| Figure 3:Flagette rash over back, legs, arms and trunk after bleomycin therapy

| Figure 4:Subsidence of rash after treatment with bleomycin withdrawal and topical steroid application
Discussion
Flagellate dermatitis is the occurrence of multiple whipped out lesions over multiple body areas. The term “Flagellate” is derived from latin word “flagellum” referring to characteristic whip like the appearance of the eruption.[3] It has been reported previously in association with a wide variety of factors including autoimmune disorders such as dermatomyositis and adult-onset Still's disease, infection with human immunodeficiency virus, toxins-like in case of consumption of shiitake mushroom, and some chemotherapeutic agents such as bleomycin, peplomycin, and docetaxel.[4] Recently, occurrence of flagellate dermatitis after bendamustine therapy has been described in a case report from the USA in one patient with chronic lymphatic leukemia by Mahmoud and Eide.[5] Peplomycin is a bleomycin derivative with reduced pulmonary toxicity that is used for lymphomas and prostatic carcinoma and has also been implicated in flagellate erythema by mechanisms similar to bleomycin.[4]
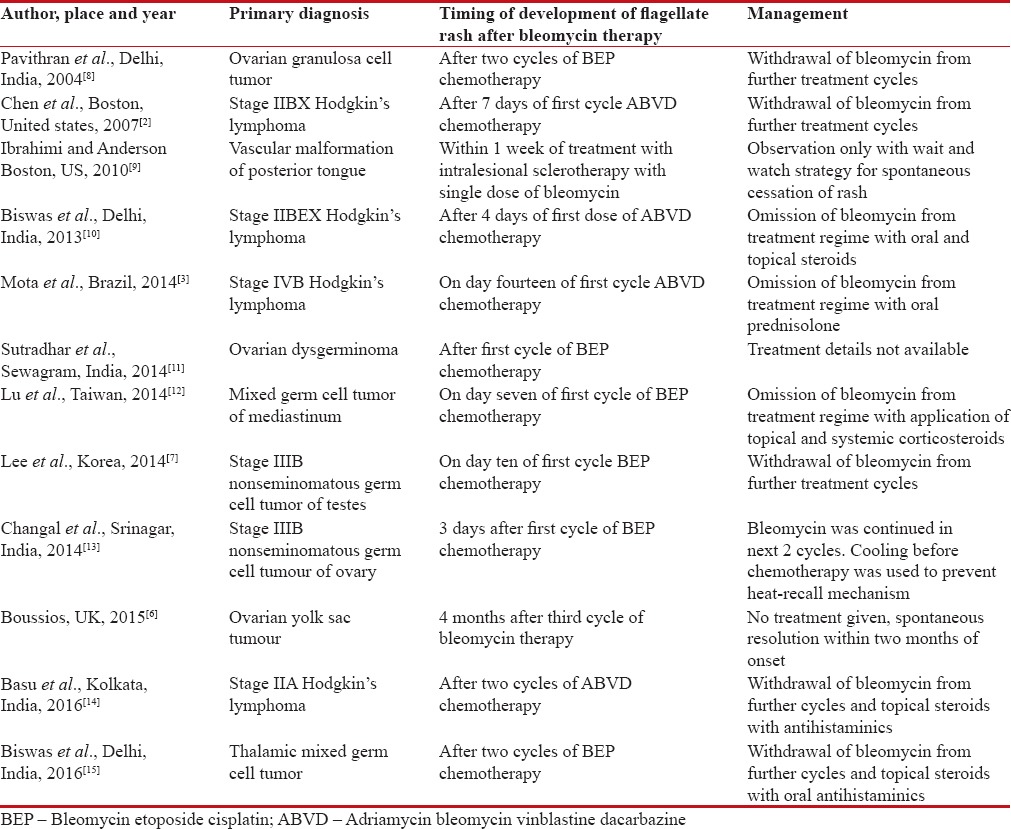
Bleomycin is an antineoplastic agent belonging to glycopeptides group and is inactivated by enzyme bleomycin hydrolase which is deficient in the skin and considerably less in concentration in the lungs leading to an increased cutaneous concentration of bleomycin in these tissues. The common mucocutaneous lesions described as a side effect of bleomycin therapy are pigmentation (~50%), alopecia (~50%), and flagellate dermatitis (8%–66%).[4] Flagellate erythema as a cutaneous manifestation of bleomycin therapy was first described in 1970.[6] The exact pathogenesis of bleomycin-induced flagellate dermatitis is still unknown and different other theories have been proposed for the same like micro-trauma, inflammatory oncotaxis, increased melanogenesis, heat recall, and reduced epidermal turnover allowing prolonged melanocytes – keratinocyte contact.[4] It is usually dose dependent and a reaction as a result of bleomycin irrespective of the route of administration or malignancy being treated and usually occurs after a cumulative dose of 90–285 mg, but some cases have been reported with doses as low as 15 mg given parenterally.[7,8] It follows the administration of bleomycin by a duration ranging from day 1 to 9 weeks and may persist for up to 6 months.[8] Previous reports have also described its occurrence even with a single dose of intralesional bleomycin used for sclerotherapy.[9] The course of bleomycin induced flagellate erythema is varied. The patient can be asymptomatic or may present with a prodrome of generalized pruritus within hours to weeks of bleomycin administration and the subsequent appearance of erythematous linear streaks which progress to typical flagellate hyperpigmentation.[7] Lesions lacks specific distribution and can occur anywhere over face, neck and trunk. Histopathologically, a spectrum of morphological findings can be seen on including urticarial hypersensitivity reaction, localized increase in melanogenesis from hyperactive and enlarged melanocytes, inflammatory oncotaxis, and lymphocytic vasculitis.[7] Salient features of different cases of bleomycin causing a flagellate rash with different doses, different routes of administration and management previously reported in the literature are summarized in Table 1.
Table 1
Previous reports of bleomycin causing flagellate rash with different doses, different routes of administration, and management reported in literature
|
Our patient noticed bleomycin-induced flagellate rash after 3 cycles of chemotherapy (total cumulative dose of 270 units) which was first noticed over the trunk and then gradually spread over other body parts. The lesion was pruritic in our patient also as were previously reported. There is no specific treatment, but avoidance of bleomycin leads to eventual clearance over months to years. However, re-exposure may produce an aggravated reaction. The patient has shown a good response to topical steroids and withdrawal of bleomycin from subsequent chemotherapy cycles.[15]
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Reinert T, Baldotto CS, Pereira Nunes FA, De Souza Scheliga AA. Bleomycin-induced lung injury. J Cancer Res 2013;9.
- Chen YB, Rahemtullah A, Breeden E, Hochberg EP. Bleomycin-induced flagellate erythema. J Clin Oncol 2007;25:898-900.
- Mota GD, Penna AM, Soares RC, Baiocchi OC. Bleomycin-induced flagellate dermatitis. Rev Bras Hematol Hemoter 2014;36:297-9.
- Bhushan P, Manjul P, Baliyan V. Flagellate dermatoses. Indian J Dermatol Venereol Leprol 2014;80:149-52.
- Mahmoud BH, Eide MJ. Bendamustine-induced “flagellate dermatitis”. Dermatol Online J 2012;18.
- Boussios S, Moschetta M, McLachlan J, Banerjee S. Bleomycin-induced flagellate erythema in a patient diagnosed with ovarian Yolk Sac tumor. Case Rep Oncol Med 2015;2015:574708.
- Lee HY, Lim KH, Ryu Y, Song SY. Bleomycin-induced flagellate erythema: A case report and review of the literature. Oncol Lett 2014;8:933-5.
- Pavithran K, Doval DC, Talwar V, Vaid AK. Flagellate hyperpigmentation from bleomycin. Indian J Dermatol Venereol Leprol 2004;70:46-7.
- Ibrahimi OA, Anderson RR. Images in clinical medicine. Bleomycin-induced flagellate hyperpigmentation. N Engl J Med 2010;363:e36.
- Biswas A, Chaudhari PB, Sharma P, Singh L, Julka PK, Sethuraman G. Bleomycin induced flagellate erythema: Revisiting a uniquecomplication. J Cancer Res Ther 2013;9:500-3.
- Sutradhar S, Kar S, Varma SK, Madke B. Bleomycin-induced flagellate hyperpigmentation: Clinical image. J Mahatma Gandhi Inst Med Sci 2014;19:72.
- Lu CC, Lu YY, Wang QR, Wu CH. Bleomycin-induced flagellate erythema. Balkan Med J 2014;31:189-90.
- Changal KH, Raina H, Changal QH, Raina M. Bleomycin-induced flagellate erythema: A rare and unique drug rash. West Indian Med J 2014;63:807-9.
- Basu D, Podder I, Das A. Bleomycin-induced flagellate hyperpigmentation: A case report with review of literature. Pigment Int 2016;3:40.
- Biswas A, Julka PK. Bleomycin induced flagellate erythema in a patient with thalamic mixed germ cell tumour: Report of a rare adverse effect. J Egypt Natl Canc Inst 2016;28:129-32.
| Figure 1:Histopathology slides showing mature cystic teratoma with Intratubular germ cell neoplasia
| Figure 2:Contrast-enhanced computed tomography abdomen chest showing multiple bilateral lung nodules with mediastinal and hilar lymphadenopathy
| Figure 3:Flagette rash over back, legs, arms and trunk after bleomycin therapy
| Figure 4:Subsidence of rash after treatment with bleomycin withdrawal and topical steroid application
References
- Reinert T, Baldotto CS, Pereira Nunes FA, De Souza Scheliga AA. Bleomycin-induced lung injury. J Cancer Res 2013;9.
- Chen YB, Rahemtullah A, Breeden E, Hochberg EP. Bleomycin-induced flagellate erythema. J Clin Oncol 2007;25:898-900.
- Mota GD, Penna AM, Soares RC, Baiocchi OC. Bleomycin-induced flagellate dermatitis. Rev Bras Hematol Hemoter 2014;36:297-9.
- Bhushan P, Manjul P, Baliyan V. Flagellate dermatoses. Indian J Dermatol Venereol Leprol 2014;80:149-52.
- Mahmoud BH, Eide MJ. Bendamustine-induced “flagellate dermatitis”. Dermatol Online J 2012;18.
- Boussios S, Moschetta M, McLachlan J, Banerjee S. Bleomycin-induced flagellate erythema in a patient diagnosed with ovarian Yolk Sac tumor. Case Rep Oncol Med 2015;2015:574708.
- Lee HY, Lim KH, Ryu Y, Song SY. Bleomycin-induced flagellate erythema: A case report and review of the literature. Oncol Lett 2014;8:933-5.
- Pavithran K, Doval DC, Talwar V, Vaid AK. Flagellate hyperpigmentation from bleomycin. Indian J Dermatol Venereol Leprol 2004;70:46-7.
- Ibrahimi OA, Anderson RR. Images in clinical medicine. Bleomycin-induced flagellate hyperpigmentation. N Engl J Med 2010;363:e36.
- Biswas A, Chaudhari PB, Sharma P, Singh L, Julka PK, Sethuraman G. Bleomycin induced flagellate erythema: Revisiting a uniquecomplication. J Cancer Res Ther 2013;9:500-3.
- Sutradhar S, Kar S, Varma SK, Madke B. Bleomycin-induced flagellate hyperpigmentation: Clinical image. J Mahatma Gandhi Inst Med Sci 2014;19:72.
- Lu CC, Lu YY, Wang QR, Wu CH. Bleomycin-induced flagellate erythema. Balkan Med J 2014;31:189-90.
- Changal KH, Raina H, Changal QH, Raina M. Bleomycin-induced flagellate erythema: A rare and unique drug rash. West Indian Med J 2014;63:807-9.
- Basu D, Podder I, Das A. Bleomycin-induced flagellate hyperpigmentation: A case report with review of literature. Pigment Int 2016;3:40.
- Biswas A, Julka PK. Bleomycin induced flagellate erythema in a patient with thalamic mixed germ cell tumour: Report of a rare adverse effect. J Egypt Natl Canc Inst 2016;28:129-32.