 PDF
PDF  Views
Views  Share
Share


Is antenatal detection of Wilms? tumor a bad prognostic marker?
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2011; 32(04): 214-216
DOI: DOI: 10.4103/0971-5851.95144
Abstract
Antenatal detection of Wilms′ tumor is rare and only nine cases have been reported till now in the English literature. We report a case of a 7-month-old child with prenatally detected renal mass managed by nephroureterectomy associated with intraoperative spill. The child developed recurrence while on DD4A chemotherapy. Salvage chemotherapy was initiated but there was no response after two cycles and the child expired due to tumor rupture.
Publication History
Article published online:
06 August 2021
© 2011. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Abstract
Antenatal detection of Wilms’ tumor is rare and only nine cases have been reported till now in the English literature. We report a case of a 7-month-old child with prenatally detected renal mass managed by nephroureterectomy associated with intraoperative spill. The child developed recurrence while on DD4A chemotherapy. Salvage chemotherapy was initiated but there was no response after two cycles and the child expired due to tumor rupture.
INTRODUCTION
Wilms’ tumor is the most common renal malignancy in children and occurs predominantly between 1 and 4 years of age. Detection of Wilms’ tumor in neonates is uncommon while antenatal detection is extremely rare. This subset of tumors is supposed to have extremely good prognosis similar to other neonatal Wilms’ tumors.[1] We report a case of prenatally detected Wilms’ tumor managed by us.
CASE REPORT
A 7-month-old boy presented with an abdominal mass since birth which gradually increased in size to occupy nearly whole of abdomen. There was no history of hematuria. Antenatal history revealed that a left renal mass had been detected on ultrasound at 7 months of gestation [Figure 1] and the child was discharged on day 3 of life without further investigations.
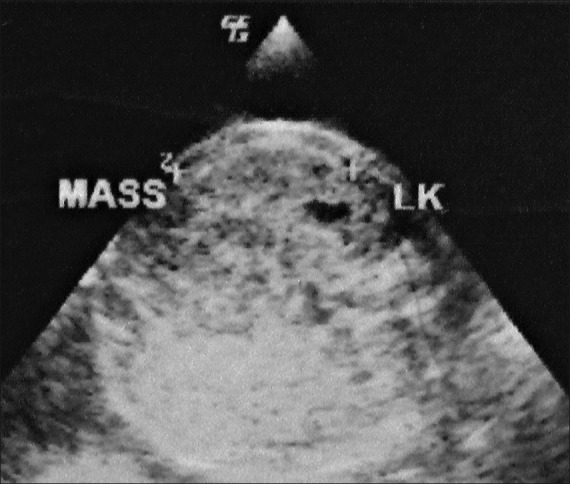
| Figure 1:Antenatal ultrasound reveals a mass in the left kidney
On examination, the child had a poor general condition and was malnourished. There was distension of abdomen due to the large intraabdominal mass. Ultrasound of the abdomen revealed a predominantly cystic 16 cm × 13 cm × 10 cm left renal mass and the findings were confirmed by contrast-enhanced computed tomography [Figure 2]. The right kidney and the inferior vena cava were normal. The chest radiograph showed clear lung fields with the pushed up diaphragm. Fine needle aspiration cytology (FNAC) was not performed as the mass was predominantly cystic. A provisional diagnosis of the cystic renal tumor was made and the child was taken up for nephroureterectomy. Exploratory laparotomy revealed a large primarily cystic left renal mass with no evident extracapsular extension or lymphadenopathy [Figure 3]. Left nephroureterectomy with lymph node sampling was performed but despite careful tissue handling, inadvertent tumor spill occurred due to rupture of cystic lesion with extremely thin walls. Right kidney did not have any gross lesion. Histopathological examination demonstrated a favorable histology triphasic Wilms’ tumor with rhabdomyoblastic differentiation [Figure 4]. A final diagnosis of stage III left Wilms’ tumor was made and the child was started on DD4A (vincristine, actinomycin D, and adriamycin) chemotherapy regimen of NWTS adjusted for age and abdominal irradiation was planned. Before the child could receive radiotherapy, a nodule at the incision site and abdomen distension was noticed when the child was admitted for the third cycle of chemotherapy [Figure 5]. The FNAC from the incision site nodule revealed a small round cell suggestive of blastemal cells [Figure 6]. The contrast-enhanced CT scan of abdomen showed a large heterogenous mass filling almost whole of abdominal cavity with involvement of the retroperitoneal and the pelvic regions. Contrast-enhanced CT scan of chest was normal. The child was subsequently started on salvage chemotherapy which consisted of ifosfamide, carboplatin, and etoposide (ICE) at age-adjusted dose. The child tolerated the chemotherapy poorly and needed prolonged GM-CSF administration because of pancytopenia. There was a little decrease in the size of the mass after completion of two cycles of chemotherapy and the child presented with a sudden increase in abdominal distension, severe pallor and shock. Abdominal ultrasonography revealed gross ascitis probably due to tumor rupture. The child expired despite active resuscitation.
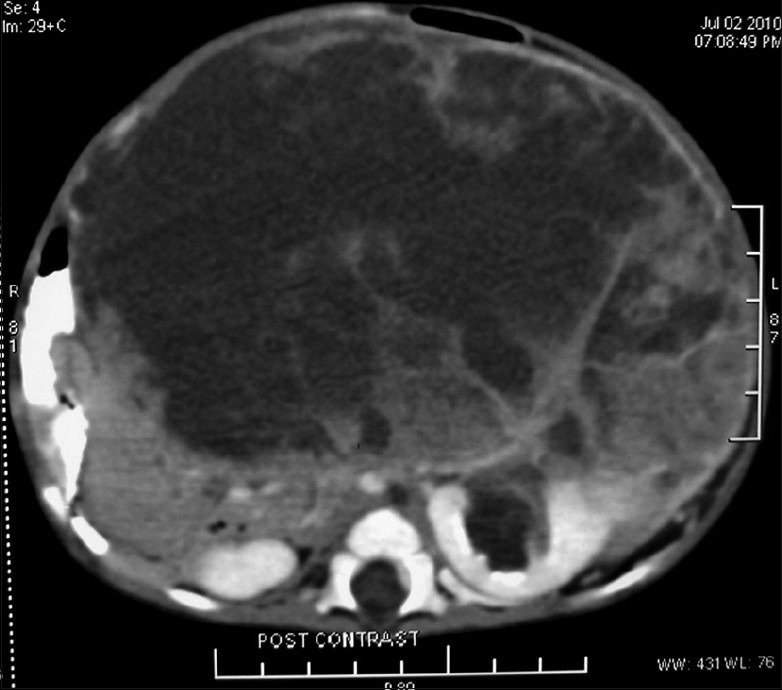
| Figure 2:Axial section of the contrast-enhanced CT scan of the abdomen shows a large predominantly cystic left renal mass
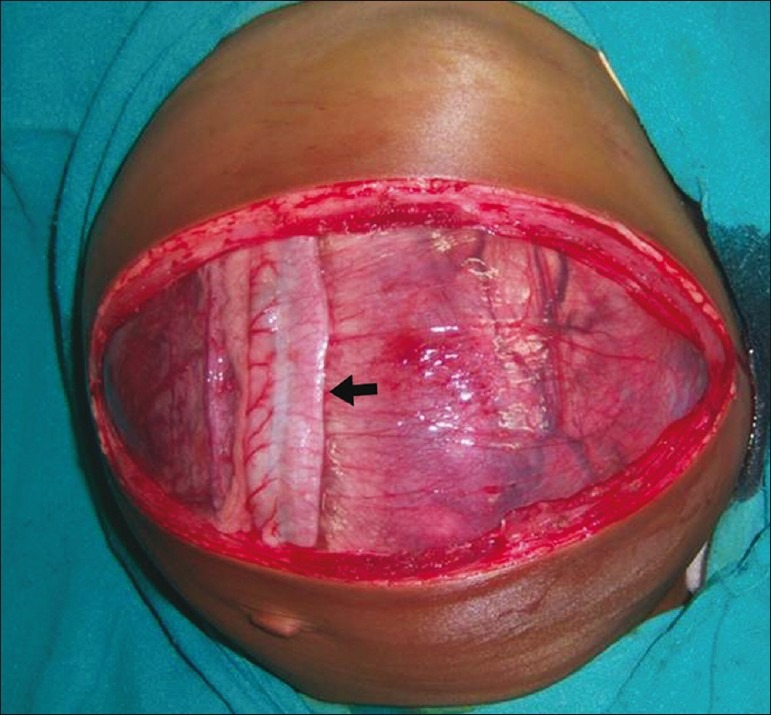
| Figure 3:Intraoperative image confirms a large renal mass displacing the descending colon (black arrow) to the right
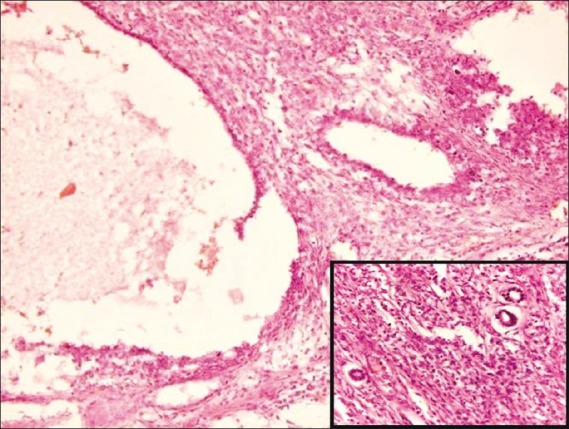
| Figure 4:Histopathological examination (hematoxyloin and eosin staining ×100) reveals cystic areas with intervening solid areas in the tumor. The inset (×250) shows blastemal and epithelial component within the solid areas

| Figure 5:Clinical photograph of the child after relapse shows a distended abdomen with a nodule at the incision site
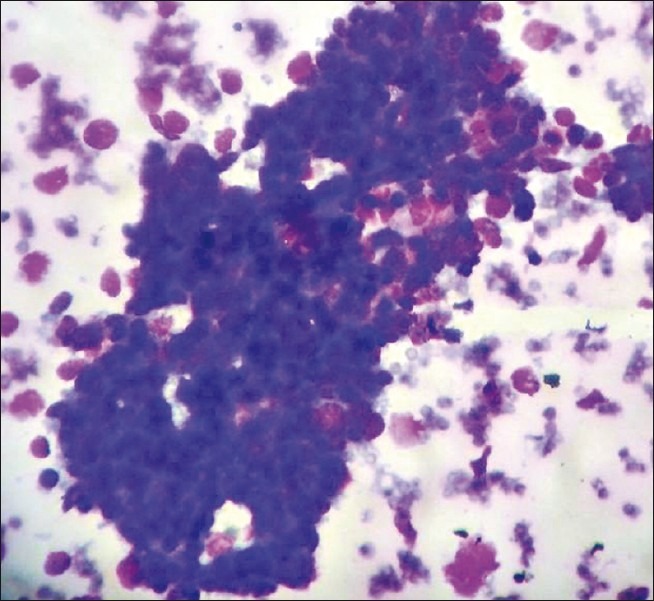
| Figure 6:Cytological examination of the aspirate from the nodule reveals the presence of small round blue cells
DISCUSSION
Wilms’ tumor is the most common renal malignancy in children but presentation in infancy is uncommon. Glick et al. reported only 11 patients under 6 months of age out of 101 children with renal tumors.[2] Most of these were diagnosed as congenital mesoblastic nephroma; and Wilms’ tumor was present in only three out of these 11 children. Of the 6,832 children registered in the NWTS from 1969 to 1993, only 11 children had neonatal Wilms’ tumor which represents a 0.16% of incidence of neonatal Wilms’ tumor.[1] Antenatal detection of Wilms’ tumor is very rare and only nine cases have been reported till now.[1–7]
The index case was prenatally detected to have a renal mass at a primary health center in a peripheral village but no follow-up was done. The child presented to us after 7 months with advanced disease. After initial evaluation of the child, surgical exploration was favored instead of a preoperative chemotherapy as the mass was primarily cystic and was rapidly increasing leading to respiratory compromise. As the histopathology report suggested the lesion to be Wilms’ tumor, the lesion was upstaged to stage III in view of the intraoperative spill, and DD4A chemotherapy initiated and radiotherapy referral sought. The frequency of abdominal recurrence from spilled cells with chemotherapy and no radiotherapy is 13.3% and the addition of 10 Gy or 20 Gy decreases the likelihood of failure of local treatment to 3- and 12-fold, respectively.[8] The failure to receive radiotherapy in our patient due to logistic reasons could have been a contributory factor for the adverse outcome. The salvage therapy consisted of ifosfamide, carboplatin and etoposide as these drugs have been reported to be effective in high risk and recurrent Wilms’ tumor.[9,10]
It has been reported that neonates with Wilms’ tumor with tumor weight less than 550 g are considered to have good prognosis and may not need even chemotherapy.[11] However of five cases of prenatally detected Wilms’ tumor in whom adequate follow-up was present, three children died. Of these three deaths, two were attributed to hydrops and one to recurrence.[1,2,6] The cause of such rapid progression of disease in our patient is difficult to point but was probably due to the unusually aggressive tumor coupled with delayed presentation and lack of radiotherapy.
Wilms’ tumor should be considered in differential diagnosis of prenatally detected renal mass and actively investigated in the postnatal period. Wilms’ tumor in infants is considered to have good prognosis but the subset of prenatally detected Wilms’ tumor may have a comparatively adverse prognosis.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- Ritchey ML, Azizkhan RG, Beckwith JB, Hrabovsky EE, Haase GM. Neonatal Wilms tumor. J Pediatr Surg 1995;30:856-9.
- Glick RD, Hicks MJ, Nuchtern JG, Wesson DE, Olutoye OO, Cass DL. Renal tumors in infants less than 6 months of age. J Pediatr Surg 2004;39:522-5.
- Tomá P, Lucigrai G, Dodero P, Lituania M. Prenatal detection of an abdominal mass by MR imaging performed while the fetus is immobilized with pancuronium bromide. AJR Am J Roentgenol 1990;154:1049-50.
- Suresh I, Suresh S, Arumugam R, Govindarajan M, Reddy MP, Sulochana NV. Antenatal diagnosis of Wilms tumor. J Ultrasound Med 1997;16:69-72.
- Applegate KE, Ghei M, Perez-Atayde AR. Prenatal detection of a Wilms′ tumor. Pediatr Radiol 1999;29:65-7.
- Vadeyar S, Ramsay M, James D, O′Neill D. Prenatal diagnosis of congenital Wilms′ tumor (nephroblastoma) presenting as fetal hydrops. Ultrasound Obstet Gynecol 2000;16:80-3.
- Linam LE, Yu X, Calvo-Garcia MA, Rubio EI, Crombleholme TM, Bove K, et al. Contribution of magnetic resonance imaging to prenatal differential diagnosis of renal tumors: Report of two cases and review of the literature. Fetal Diagn Ther 2010;28:100-8.
- Kalapurakal JA, Li SM, Breslow NE, Beckwith JB, Ritchey ML, Shamberger RC, et al. Intraoperative spillage of favorable histology Wilms tumor cells: Influence of irradiation and chemotherapy regimens on abdominal recurrence. A report from the National Wilms Tumor Study Group. Int J Radiat Oncol Biol Phys 2010;76:201-6.
- Tournade MF, Lemerle J, Brunat-Mentigny M, Bachelot C, Roche H, Taboureau O, et al. Ifosfamide is an active drug in Wilms′ tumor: A phase II study conducted by the French Society of Pediatric Oncology. J Clin Oncol 1988;6:793-6.
- Pein F, Tournade MF, Zucker JM, Brunat-Mentigny M, Deville A, Boutard P, et al. Etoposide and carboplatin: A highly effective combination in relapsed or refractory Wilms′ tumor-a phase II study by the French Society of Pediatric Oncology. J Clin Oncol 1994;12:931-6.
- Shamberger RC, Anderson JR, Breslow NE, Perlman EJ, Beckwith JB, Ritchey ML, et al. Long-term outcomes for infants with very low risk Wilms tumor treated with surgery alone in National Wilms Tumor Study-5. Ann Surg 2010;251:555-8.
| Figure 1:Antenatal ultrasound reveals a mass in the left kidney
| Figure 2:Axial section of the contrast-enhanced CT scan of the abdomen shows a large predominantly cystic left renal mass
| Figure 3:Intraoperative image confirms a large renal mass displacing the descending colon (black arrow) to the right
| Figure 4:Histopathological examination (hematoxyloin and eosin staining ×100) reveals cystic areas with intervening solid areas in the tumor. The inset (×250) shows blastemal and epithelial component within the solid areas
| Figure 5:Clinical photograph of the child after relapse shows a distended abdomen with a nodule at the incision site
| Figure 6:Cytological examination of the aspirate from the nodule reveals the presence of small round blue cells
References
- Ritchey ML, Azizkhan RG, Beckwith JB, Hrabovsky EE, Haase GM. Neonatal Wilms tumor. J Pediatr Surg 1995;30:856-9.
- Glick RD, Hicks MJ, Nuchtern JG, Wesson DE, Olutoye OO, Cass DL. Renal tumors in infants less than 6 months of age. J Pediatr Surg 2004;39:522-5.
- Tomá P, Lucigrai G, Dodero P, Lituania M. Prenatal detection of an abdominal mass by MR imaging performed while the fetus is immobilized with pancuronium bromide. AJR Am J Roentgenol 1990;154:1049-50.
- Suresh I, Suresh S, Arumugam R, Govindarajan M, Reddy MP, Sulochana NV. Antenatal diagnosis of Wilms tumor. J Ultrasound Med 1997;16:69-72.
- Applegate KE, Ghei M, Perez-Atayde AR. Prenatal detection of a Wilms′ tumor. Pediatr Radiol 1999;29:65-7.
- Vadeyar S, Ramsay M, James D, O′Neill D. Prenatal diagnosis of congenital Wilms′ tumor (nephroblastoma) presenting as fetal hydrops. Ultrasound Obstet Gynecol 2000;16:80-3.
- Linam LE, Yu X, Calvo-Garcia MA, Rubio EI, Crombleholme TM, Bove K, et al. Contribution of magnetic resonance imaging to prenatal differential diagnosis of renal tumors: Report of two cases and review of the literature. Fetal Diagn Ther 2010;28:100-8.
- Kalapurakal JA, Li SM, Breslow NE, Beckwith JB, Ritchey ML, Shamberger RC, et al. Intraoperative spillage of favorable histology Wilms tumor cells: Influence of irradiation and chemotherapy regimens on abdominal recurrence. A report from the National Wilms Tumor Study Group. Int J Radiat Oncol Biol Phys 2010;76:201-6.
- Tournade MF, Lemerle J, Brunat-Mentigny M, Bachelot C, Roche H, Taboureau O, et al. Ifosfamide is an active drug in Wilms′ tumor: A phase II study conducted by the French Society of Pediatric Oncology. J Clin Oncol 1988;6:793-6.
- Pein F, Tournade MF, Zucker JM, Brunat-Mentigny M, Deville A, Boutard P, et al. Etoposide and carboplatin: A highly effective combination in relapsed or refractory Wilms′ tumor-a phase II study by the French Society of Pediatric Oncology. J Clin Oncol 1994;12:931-6.
- Shamberger RC, Anderson JR, Breslow NE, Perlman EJ, Beckwith JB, Ritchey ML, et al. Long-term outcomes for infants with very low risk Wilms tumor treated with surgery alone in National Wilms Tumor Study-5. Ann Surg 2010;251:555-8.