 PDF
PDF  Views
Views  Share
Share


Massive Hemoptysis: A Rare Presentation of Anterior Mediastinal Teratoma in an Adolescent
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2017; 38(02): 215-217
DOI: DOI: 10.4103/ijmpo.ijmpo_62_16
Abstract
Germ cell tumors are predominantly found in the gonads, and the most common extragonadal site is anterior mediastinum. Usual symptoms are cough, dyspnea, and fever, chest pain due to mass effect or intrapulmonary invasion but hemoptysis is rare and may result from either communication with tracheobronchial tree or may result from bronchial bleeding due to irritation by tumor. As in our case, patient presenting with massive hemoptysis and shock are the rarest presentation of a benign teratoma.
Publication History
Article published online:
06 July 2021
© 2017. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Abstract
Germ cell tumors are predominantly found in the gonads, and the most common extragonadal site is anterior mediastinum. Usual symptoms are cough, dyspnea, and fever, chest pain due to mass effect or intrapulmonary invasion but hemoptysis is rare and may result from either communication with tracheobronchial tree or may result from bronchial bleeding due to irritation by tumor. As in our case, patient presenting with massive hemoptysis and shock are the rarest presentation of a benign teratoma.
Introduction
Hemoptysis is defined as the expectoration of blood or blood-tinged sputum from the lower respiratory tract. Although common in adult, blood-tinged sputum is rare presenting symptoms in children. Most commonly hemoptysis in children is caused by bronchiectasis, pulmonary tuberculosis, foreign body aspiration, congenital foreign body, and rarely malignancy.[1] Germ cell tumors are predominantly found in the gonads, and the most common extragonadal site is anterior mediastinum. Mediastinal germ cell tumors account for 24% in children. Patients with mediastinum tumors are usually discovered incidentally on chest radiograph.[2,3] Most symptoms are due to mass effect and pulmonary involvement.[4] Here, we report a case of benign teratoma which was presented with massive hemoptysis along with hemorrhagic shock an unusual presentation in pediatric age group.
Case Report
A 10-year-old female child was admitted to Pediatric Intensive Care Unit through Emergency Department with a history of two to three episodes of massive hemoptysis for the past 2 days. She had such intermittent episode of hemoptysis for the past 2 months. She had no fever, breathlessness, loss of weight, joint pain, or renal symptoms. She had no significant past or family history of tuberculosis. On arrival in Emergency Department, she was in hemorrhagic shock. The patient was resuscitated with fluid, and whole blood transfusion was given.
Her investigation yielded hemoglobin was 4 gm% with normocytic normochromic type of anemia, an erythrocyte sedimentation rate of 20 mm at end of 1t hour. Her total leukocyte count and differential leukocyte count were within normal limits, while her tuberculin test was negative. Chest radiograph was suggestive of well-circumscribed mass on upper left side with infective changes [Figure 1]. High-resolution computed tomography (CT) thorax revealed infective changes in both lung fields with well-circumscribed mass of size 4 cm × 4 cm × 4 cm on the left main bronchus and extending on lingual lobe suggestive of thymolipoma [Figure 2]. CT-guided fine-needle aspiration cytology shows fat cells. Intraoperatively, there was a mass of size 4 cm × 4 cm × 4 cm in the anterior mediastinum and communicating with left main bronchus and lingual lobe with cheesy puttaceous material coming out of it and adhere to aorta, pericardium, and pleura. Mass was excised, and partial lobectomy was done. Histopathologically, on cut surface, mass was solid grayish white in color with many cysts of size 1 cm × 1 cm × 1 cm filled with brownish friable material and yellowish fatty area. On microscopy, elements of all three germ layer namely epidermis, skin adnexal structure, adipose tissues in sheets and groups, mature cartilage, muscle tissues, and respiratory epithelium suggestive of mature teratoma were seen [Figures [Figures33 and and44].

| Figure 1:Chest radiograph shows well-circumscribed mass in mediastinum

| Figure 2:Computed tomography thorax shows well-circumscribed mass in mediastinum
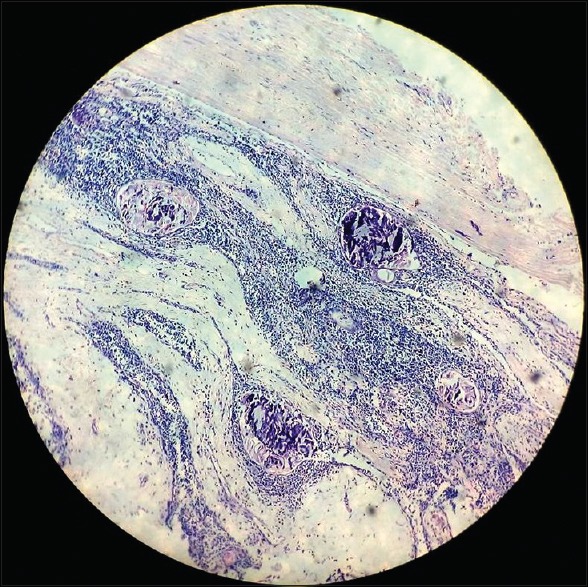
| Figure 3:Microscopic changes of mature teratoma [Low power]
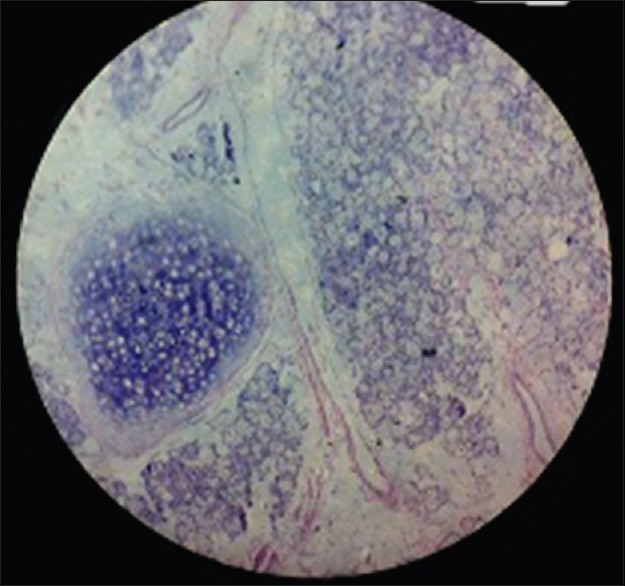
| Figure 4:Microscopic changes of mature teratoma [High power]
Discussion
Anterior mediastinum is the most common extragonadal site of germ cell tumor and accounting 24% of all pediatric anterior mediastinal tumors.[2] Benign lesions have no sex predilection; however, malignant ones are more common in males.[5] A theory to account for extragonadal germ cell tumor was proposed by Fine et al.,[6] who suggests that there was an error in the migration of primitive germ cells along the urogenital ridge.
Mediastinal tumors rarely produce symptoms except when they attain large size or rupture into lung and bronchial tree, pleural space, pericardial space, or great vessels.[5] Most mediastinal teratomas with pulmonary involvement have, for unknown reasons, a predilection for the left upper lobe.[4] Our case is also having left upper lobe and lingual lobe involvement. Unusual but pathognomonic symptom of expectoration of hair (trichoptysis) is extremely rare in pediatric practice. Usual symptoms are cough, dyspnea, and fever, chest pain due to mass effect or intrapulmonary invasion but hemoptysis is rare and may result from either communication with tracheobronchial tree or may result from bronchial bleeding due to irritation by tumor.[4] Here, we report a case of benign teratoma which was presented with massive hemoptysis along with hemorrhagic shock an unusual presentation in pediatric age group. All these symptoms may mimic pulmonary tuberculosis in adolescent, especially in tuberculosis-endemic area; but in our patient, tuberculosis workup was negative. Teratomas can get infected from contagious foci in the lung parenchyma or through blood stream resulting into bronchopneumonia, lung abscess, or emphysema.[7] Similar infective changes in both lungs were noted in our case.
Complete curative surgical removal of mediastinal teratomas is the treatment of choice, as it established the diagnosis and prevent life-threatening complication.
Conclusion
Massive hemoptysis is the rarest and life-threatening complication in pulmonary tuberculosis, coagulopathy, and leukemias; but mediastinal teratomas is the rarest cause of massive hemoptysis in pediatric practice.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Gaude GS. Hemoptysis in children. Indian Pediatr 2010;47:245-54.
- Yalagachin GH. Anterior mediastinal teratoma – A case report with review of literature. Indian J Surg 2013;75 Suppl 1:182-4.
- Duwe BV, Sterman DH, Musani AI. Tumors of the mediastinum. Chest 2005;128:2893-909.
- Chen RF, Chang TH, Chang CC, Lee CN. Mediastinal teratoma with pulmonary involvement presenting as massive hemoptysis in 2 patients. Respir Care 2010;55:1094-6.
- Badar F, Yasmeen S, Afroz N, Khan N, Azfar SF. Benign mediastinal teratoma with intrapulmonary and bronchial rupture presenting with recurrent hemoptysis. Iran J Radiol 2013;10:86-9.
- Fine G, Smith RW Jr., Pachter MR. Primary extragenital choriocarcinoma in the male subject. Case report and review of the literature. Am J Med 1962;32:776-94.
- Bhatt G, Nandan D, Sen A, Kanaujia P. Fever of unknown origin: A case of post obstructive pneumonia complicating mature teratoma. Ann Med Health Sci Res 2013;3:461-3.
| Figure 1:Chest radiograph shows well-circumscribed mass in mediastinum
| Figure 2:Computed tomography thorax shows well-circumscribed mass in mediastinum
| Figure 3:Microscopic changes of mature teratoma [Low power]
| Figure 4:Microscopic changes of mature teratoma [High power]
References
- Gaude GS. Hemoptysis in children. Indian Pediatr 2010;47:245-54.
- Yalagachin GH. Anterior mediastinal teratoma – A case report with review of literature. Indian J Surg 2013;75 Suppl 1:182-4.
- Duwe BV, Sterman DH, Musani AI. Tumors of the mediastinum. Chest 2005;128:2893-909.
- Chen RF, Chang TH, Chang CC, Lee CN. Mediastinal teratoma with pulmonary involvement presenting as massive hemoptysis in 2 patients. Respir Care 2010;55:1094-6.
- Badar F, Yasmeen S, Afroz N, Khan N, Azfar SF. Benign mediastinal teratoma with intrapulmonary and bronchial rupture presenting with recurrent hemoptysis. Iran J Radiol 2013;10:86-9.
- Fine G, Smith RW Jr., Pachter MR. Primary extragenital choriocarcinoma in the male subject. Case report and review of the literature. Am J Med 1962;32:776-94.
- Bhatt G, Nandan D, Sen A, Kanaujia P. Fever of unknown origin: A case of post obstructive pneumonia complicating mature teratoma. Ann Med Health Sci Res 2013;3:461-3.