 PDF
PDF  Views
Views  Share
Share


Neurolymphomatosis: A Surreal Presentation of Lymphoma
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2017; 38(03): 287-290
DOI: DOI: 10.4103/ijmpo.ijmpo_151_16
Abstract
Background: Neurolymphomatosis is a neurologic complication poorly recognized by neurologists and oncologists and presents usually several months after successful treatment of systemic lymphoma. Other disorders that must be differentiated from these entities include peripheral-nerve or nerve root compression and paraneoplastic neuropathy. Aim: To describe the unusual occurrence of neurolymphomatosis in a patient of B-cell lymphoma. Method: Diagnosis was made by demonstration of enhancement of nerve roots on Magnetic Resonance Imaging of the brachial, lumbosacral plexus, peripheral nerves or by increased hyper-metabolic activity along the course of affected nerves on fluorodeoxyglucose positron emission tomography (FDG-PET). Results and Conclusion: MRI and PET-CT are imaging modalities of choice for evaluation of patients with lymphoma and suspected neural involvement. Treatment of neurolymphomatosis consists of focal radiotherapy and high-dose methotrexate therapy.
Keywords
Lymphoma - magnetic resonance imaging - neurolymphomatosis - positron emission tomography-computed tomography imagingPublication History
Article published online:
04 July 2021
© 2017. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Abstract
Background:
Neurolymphomatosis is a neurologic complication poorly recognized by neurologists and oncologists and presents usually several months after successful treatment of systemic lymphoma. Other disorders that must be differentiated from these entities include peripheral-nerve or nerve root compression and paraneoplastic neuropathy.
Aim:
To describe the unusual occurrence of neurolymphomatosis in a patient of B-cell lymphoma.
Method:
Diagnosis was made by demonstration of enhancement of nerve roots on Magnetic Resonance Imaging of the brachial, lumbosacral plexus, peripheral nerves or by increased hyper-metabolic activity along the course of affected nerves on fluorodeoxyglucose positron emission tomography (FDG-PET).
Results and Conclusion:
MRI and PET-CT are imaging modalities of choice for evaluation of patients with lymphoma and suspected neural involvement. Treatment of neurolymphomatosis consists of focal radiotherapy and high-dose methotrexate therapy.
Introduction
The lymphomatous infiltration of a nerve root, cranial or peripheral nerve or multiple nerves is known as neurolymphomatosis. It is a rare neurologic complication of systemic lymphoma that is poorly recognized by clinicians. It is an uncommon syndrome characterized by a direct invasion of the peripheral nervous system by lymphoma. The predominant malignant cell type is diffuse large B-cell although rare cases secondary to follicular lymphoma, peripheral T-cell lymphoma, and mantle cell lymphoma have been reported.[1,2,3]
A high index of suspicion is required as the presenting symptoms of this condition are varied (plexopathy, mononeuritis multiplex, foot drop, radiculopathy, and cranial nerve palsies). Various differential diagnoses need to be considered. These include nerve damage from herpes zoster, leptomeningeal lymphomatosis, radiation neuritis, nerve root compression, lymphoma-associated vasculitis, and paraneoplastic syndromes.[4,5]
Case Report
A 48-year-old male patient, normotensive, nondiabetic diagnosed with chronic lymphocytic leukemia (flow cytometry proven). He was planned for six cycles of rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisolone. His pretreatment positron emission tomography-computed tomography (PET-CT) revealed multiple fluorodeoxyglucose (FDG) avid hypermetabolic lymph nodes in both supra- and infra-diaphragmatic regions [Figure 1].
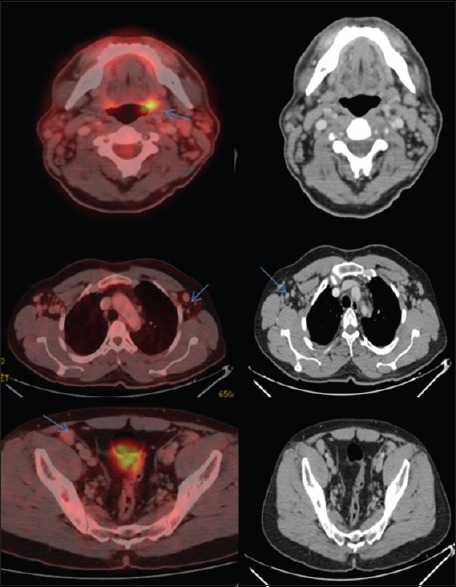
| Figure 1:Positron emission tomography-computed tomography scan dated May 23, 2015 revealed multiple fluorodeoxyglucose avid hypermetabolic lymph nodes in both supra- and infra-diaphragmatic regions
After three cycles of chemotherapy, a follow-up PET scan (October 5, 2015) was done to assess interval changes. There was significant regression in size and metabolic activity of the lymph nodes (Category III Deauville score) suggesting a good response to treatment [Figure 2].

| Figure 2:Follow-up positron emission tomography scan dated October 5, 2015
After the fifth cycle of chemotherapy, patient had complaints of fever, dyspnea on exertion and had prolonged postchemotherapy febrile neutropenia and was admitted for treatment.
The following regression in symptoms and improving cell counts, patient was discharged.
After 10 days, patient presented with complaints of left foot drop in March 2016.
Magnetic resonance imaging (MRI) of spine and pelvis was performed. It revealed diffuse nodular and thickened nerve roots at L4, L5, S1, and S2 more marked on the left side extending up to greater sciatic foramen (better appreciated on T2/short-tau inversion recovery [STIR] axial and coronal images) [Figure 3].
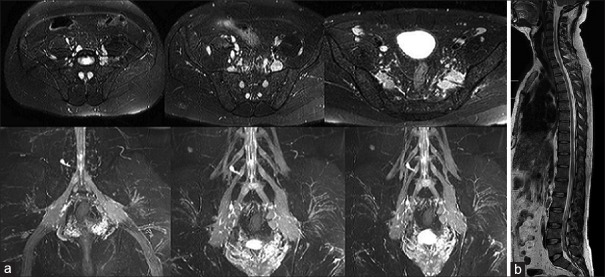
| Figure 3:(a) 3.0 Tesla magnetic resonance imaging of lumbar spine. (b) Magnetic resonance imaging -T2-weighted images sagittal plane whole spine
No evident disc herniation, epidural soft tissue, or intrinsic cord abnormality was noted.
Similar characteristic findings were seen along left C4 and bilateral C5–C8 nerve roots [Figure 4].
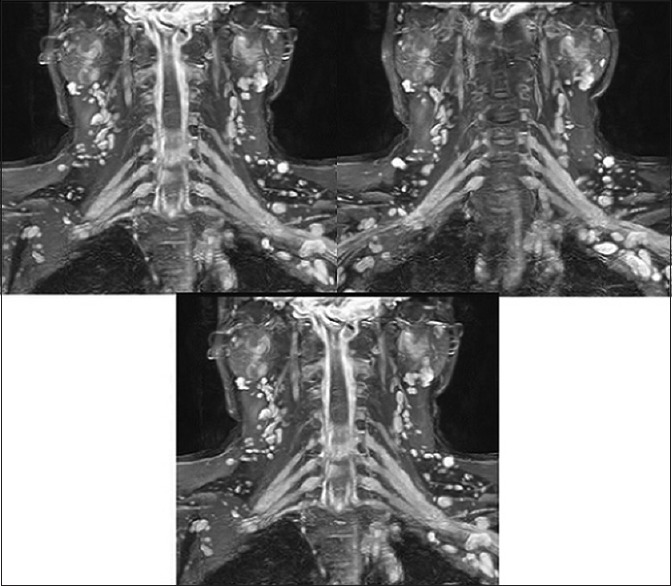
| Figure 4:(a) A case of acute myeloid leukemia with inv 16 showing the presence of abnormal eosinophils in addition to usual morphological features of myelomonocytic leukemia. (b) Monocytic nature of the blasts being highlighted by positive reaction with nonspecific esterase
The MRI findings with given clinical history were highly in favor of lymphomatous involvement of the brachial and lumbosacral plexus suggesting neurolymphomatosis.
Subsequent PET-CT scan done in the same week revealed moderate-grade FDG avid lymph nodes involving bilateral external iliac regions and low-grade FDG avid lymph nodes in retroperitoneum. Non-FDG avid cervical and mediastinal lymph nodes were noted.
There was seen high-grade FDG avid uptake (maximum standardized uptake value – 12) along the lumbosacral plexus more marked on the left side and along brachial plexus on either side [Figures [Figures55 and and66].
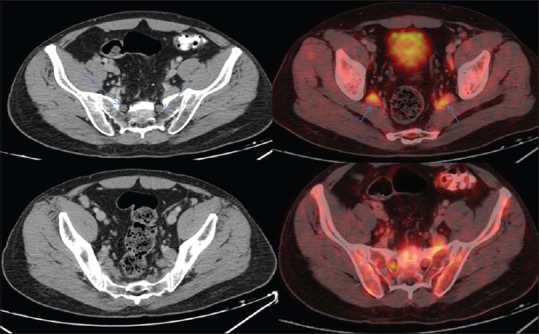
| Figure 5:PET-CT axial images reveal intense enhancement along the lumbosacral plexus.(Left>Right), as demonstrated by tht blue arrows

| Figure 6:PET CT coronal images reveal intensely enhancing lumbar plexus and brachial pleuxs (blue arrows)
Discussion
Neurolymphomatosis has a classical presentation with a painful, sensorimotor peripheral neuropathy affecting multiple limbs in an asymmetric manner. It usually presents with a relatively rapid evolution.[1,2,3] Solitary peripheral nerve involvement with or without painful neuropathy may also be seen.
The neurological complications usually present several months after ongoing treatment of systemic lymphoma. In some rare cases, it may precede the diagnosis of lymphoma and presents as the sole manifestation of lymphoma. It is frequently misdiagnosed as it has numerous differential diagnoses, namely, paraneoplastic/inflammatory neuropathy particularly if there is an initial response to steroids, peripheral nerve compression, or chemotherapy-induced peripheral neuropathy.[4,5]
CT imaging fails in demonstration of nerve root or peripheral nerve abnormalities in patients with neurolymphomatosis adding up to difficulty in making the diagnosis. MRI is the investigation of choice to demonstrate enlargement and nodularity of the peripheral nerves, brachial plexus, or the lumbosacral plexus. On STIR/T2-weighted images, infiltrated nerves appear hyperintense resonating the lymphoma and peritumoral edema.
High-grade FDG activity or hypermetabolic activity along the course of a nerve root or peripheral nerve on FDG-PET favors the diagnosis of neurolymphomatosis in patients with the appropriate clinical history and associated abnormal magnetic resonance findings.[6,7,8]
Biopsy is considered as the final diagnosis although patients with classic clinical history and abnormal PET imaging for neurolymphomatosis are usually treated empirically given the difficulty in making a histological diagnosis.[9]
MRI and FDG-PET/CT assist in identifying the target for nerve biopsy in a patient in which a biopsy is critical, especially in those without a history of lymphoma.[10,11,12,13] In cases of uncertainty, image-guided percutaneous nerve biopsy may be performed safely.
Treatment with corticosteroids may initially result in a radiographic response and improved symptoms although neurolymphomatosis typically recurs or progresses as the malignancy develops resistance. Radiotherapy is particularly useful in patients with significant neurologic dysfunction since it may rapidly improve or stabilize symptoms.[14,15,16,17,18] Given the rarity of the disease, prognosis is not well established, although limited reports suggest a poor outcome.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Grisariu S, Avni B, Batchelor TT, van den Bent MJ, Bokstein F, Schiff D, et al. Neurolymphomatosis: An International Primary CNS Lymphoma Collaborative Group report. Blood 2010;115:5005-11.
- Baehring JM, Damek D, Martin EC, Betensky RA, Hochberg FH. Neurolymphomatosis. Neuro Oncol 2003;5:104-15.
- Chamberlain MC, Fink J. Neurolymphomatosis: A rare metastatic complication of diffuse large B-Cell lymphoma. J Neurooncol 2009;95:285-8.
- Tomita M, Koike H, Kawagashira Y, Iijima M, Adachi H, Taguchi J, et al. Clinicopathological features of neuropathy associated with lymphoma. Brain 2013;136:2563-78.
- Baehring J, Cooper D. Neurolymphomatosis. J Neurooncol 2004;68:243-4.
- Trojan A, Jermann M, Taverna C, Hany TF. Fusion PET-CT imaging of neurolymphomatosis. Ann Oncol 2002;13:802-5.
- Kelly JJ, Karcher DS. Lymphoma and peripheral neuropathy: A clinical review. Muscle Nerve 2005;31:301-13.
- Beristain X, Azzarelli B. The neurological masquerade of intravascular lymphomatosis. Arch Neurol 2002;59:439-43.
- Bokstein F, Goor O, Shihman B, Rochkind S, Even-Sapir E, Metser U, et al. Assessment of neurolymphomatosis by brachial plexus biopsy and PET/CT. Report of a case. J Neurooncol 2005;72:163-7.
- Viali S, Hutchinson DO, Hawkins TE, Croxson MC, Thomas M, Allen JP, et al. Presentation of intravascular lymphomatosis as lumbosacral polyradiculopathy. Muscle Nerve 2000;23:1295-300.
- Crush AB, Howe BM, Spinner RJ, Amrami KK, Hunt CH, Johnson GB, et al. Malignant involvement of the peripheral nervous system in patients with cancer: Multimodality imaging and pathologic correlation. Radiographics 2014;34:1987-2007.
- Gan HK, Azad A, Cher L, Mitchell PL. Neurolymphomatosis: Diagnosis, management, and outcomes in patients treated with rituximab. Neuro Oncol 2010;12:212-5.
- Ogose A, Hotta T, Morita T, Higuchi T, Umezu H, Imaizumi S, et al. Diagnosis of peripheral nerve sheath tumors around the pelvis. Jpn J Clin Oncol 2004;34:405-13.
- Kanter P, Zeidman A, Streifler J, Marmelstein V, Even-Sapir E, Metser U, et al. PET-CT imaging of combined brachial and lumbosacral neurolymphomatosis. Eur J Haematol 2005;74:66-9.
- Rosso SM, de Bruin HG, Wu KL, van den Bent MJ. Diagnosis of neurolymphomatosis with FDG PET. Neurology 2006;67:722-3.
- Oztürk E, Arpaci F, Kocaoglu M, Arslan N, Bulakbasi N, Ozgüven M. Detection of widespread neurolymphomatosis with 18F-FDG PET. Eur J Nucl Med Mol Imaging 2006;33:975-6.
- Habermann TM, Weller EA, Morrison VA, et al. Rituximab-CHOP versus CHOP alone or with maintenance rituximab in older patients with diffuse large B-cell lymphoma. J Clin Oncol. 2006;24:3121-7.
- Masatoshi N, Kouhei Y, Yuji N, Shin-ichi K, Tadakazu K, Akifumi TK. Neurolymphomatosis as a manifestation of relapsed primary cardiac lymphoma. Int J of Hematology 2010;92:79-680.
| Figure 1:Positron emission tomography-computed tomography scan dated May 23, 2015 revealed multiple fluorodeoxyglucose avid hypermetabolic lymph nodes in both supra- and infra-diaphragmatic regions
| Figure 2:Follow-up positron emission tomography scan dated October 5, 2015
| Figure 3:(a) 3.0 Tesla magnetic resonance imaging of lumbar spine. (b) Magnetic resonance imaging -T2-weighted images sagittal plane whole spine
| Figure 4:(a) A case of acute myeloid leukemia with inv 16 showing the presence of abnormal eosinophils in addition to usual morphological features of myelomonocytic leukemia. (b) Monocytic nature of the blasts being highlighted by positive reaction with nonspecific esterase
| Figure 5:PET-CT axial images reveal intense enhancement along the lumbosacral plexus.(Left>Right), as demonstrated by tht blue arrows
| Figure 6:PET CT coronal images reveal intensely enhancing lumbar plexus and brachial pleuxs (blue arrows)
References
- Grisariu S, Avni B, Batchelor TT, van den Bent MJ, Bokstein F, Schiff D, et al. Neurolymphomatosis: An International Primary CNS Lymphoma Collaborative Group report. Blood 2010;115:5005-11.
- Baehring JM, Damek D, Martin EC, Betensky RA, Hochberg FH. Neurolymphomatosis. Neuro Oncol 2003;5:104-15.
- Chamberlain MC, Fink J. Neurolymphomatosis: A rare metastatic complication of diffuse large B-Cell lymphoma. J Neurooncol 2009;95:285-8.
- Tomita M, Koike H, Kawagashira Y, Iijima M, Adachi H, Taguchi J, et al. Clinicopathological features of neuropathy associated with lymphoma. Brain 2013;136:2563-78.
- Baehring J, Cooper D. Neurolymphomatosis. J Neurooncol 2004;68:243-4.
- Trojan A, Jermann M, Taverna C, Hany TF. Fusion PET-CT imaging of neurolymphomatosis. Ann Oncol 2002;13:802-5.
- Kelly JJ, Karcher DS. Lymphoma and peripheral neuropathy: A clinical review. Muscle Nerve 2005;31:301-13.
- Beristain X, Azzarelli B. The neurological masquerade of intravascular lymphomatosis. Arch Neurol 2002;59:439-43.
- Bokstein F, Goor O, Shihman B, Rochkind S, Even-Sapir E, Metser U, et al. Assessment of neurolymphomatosis by brachial plexus biopsy and PET/CT. Report of a case. J Neurooncol 2005;72:163-7.
- Viali S, Hutchinson DO, Hawkins TE, Croxson MC, Thomas M, Allen JP, et al. Presentation of intravascular lymphomatosis as lumbosacral polyradiculopathy. Muscle Nerve 2000;23:1295-300.
- Crush AB, Howe BM, Spinner RJ, Amrami KK, Hunt CH, Johnson GB, et al. Malignant involvement of the peripheral nervous system in patients with cancer: Multimodality imaging and pathologic correlation. Radiographics 2014;34:1987-2007.
- Gan HK, Azad A, Cher L, Mitchell PL. Neurolymphomatosis: Diagnosis, management, and outcomes in patients treated with rituximab. Neuro Oncol 2010;12:212-5.
- Ogose A, Hotta T, Morita T, Higuchi T, Umezu H, Imaizumi S, et al. Diagnosis of peripheral nerve sheath tumors around the pelvis. Jpn J Clin Oncol 2004;34:405-13.
- Kanter P, Zeidman A, Streifler J, Marmelstein V, Even-Sapir E, Metser U, et al. PET-CT imaging of combined brachial and lumbosacral neurolymphomatosis. Eur J Haematol 2005;74:66-9.
- Rosso SM, de Bruin HG, Wu KL, van den Bent MJ. Diagnosis of neurolymphomatosis with FDG PET. Neurology 2006;67:722-3.
- Oztürk E, Arpaci F, Kocaoglu M, Arslan N, Bulakbasi N, Ozgüven M. Detection of widespread neurolymphomatosis with 18F-FDG PET. Eur J Nucl Med Mol Imaging 2006;33:975-6.
- Habermann TM, Weller EA, Morrison VA, et al. Rituximab-CHOP versus CHOP alone or with maintenance rituximab in older patients with diffuse large B-cell lymphoma. J Clin Oncol. 2006;24:3121-7.
- Masatoshi N, Kouhei Y, Yuji N, Shin-ichi K, Tadakazu K, Akifumi TK. Neurolymphomatosis as a manifestation of relapsed primary cardiac lymphoma. Int J of Hematology 2010;92:79-680.