 PDF
PDF  Views
Views  Share
Share


Relapsed Plasmablastic Lymphoma in an HIV-Infected Patient—Experience of High-Dose Chemotherapy with Autologous Stem Cell Rescue: A Case Report with Review of Literature
CC BY-NC-ND 4.0 ? Indian J Med Paediatr Oncol
DOI: DOI: 10.1055/s-0042-1742455
Abstract
Plasmablastic lymphoma (PBL) is a subtype of non-Hodgkin lymphoma with dismal outcome despite multidrug chemotherapy regimen leading to high rates of disease recurrence. High-dose chemotherapy with autologous stem cell rescue (HDCT/ASCR) is an effective salvage therapy in patients with chemo-sensitive human immunodeficiency virus (HIV)-associated non-Hodgkin lymphoma. We report a case of 38 years old male with relapsed PBL associated with underlying HIV infection, who underwent HDCT/ASCR. He presented with low-grade fever and abdominal discomfort. He was evaluated with fluorodeoxyglucose positron emission tomography scan followed by omental biopsy that confirmed disease relapse. He received second-line therapy containing bortezomib and daratumumab and achieved remission (CR2). Subsequently, he underwent HDCT/ASCR. He has been clinically asymptomatic in good general condition having disease-free survival of 18 months after HDCT/ASCR. Our objective of presenting this case report is its complexity from presentation, diagnosis, and treatment. We take this opportunity to review the epidemiology and clinicopathological characteristics of PBL, as well as discuss the advancements in therapeutic options of this challenging disease.
Keywords
plasmablastic lymphoma - HIV infection - combined antiretroviral therapy - autologous stem cell transplantEthics
The ethics committee approval for publication (ECC/ONCO/June/28, dated: 28/06/2021) was obtained from Jaslok Hospital and Research Centre institutional ethics committee.
Publication History
18 April 2022 (online)
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Abstract
Plasmablastic lymphoma (PBL) is a subtype of non-Hodgkin lymphoma with dismal outcome despite multidrug chemotherapy regimen leading to high rates of disease recurrence. High-dose chemotherapy with autologous stem cell rescue (HDCT/ASCR) is an effective salvage therapy in patients with chemo-sensitive human immunodeficiency virus (HIV)-associated non-Hodgkin lymphoma. We report a case of 38 years old male with relapsed PBL associated with underlying HIV infection, who underwent HDCT/ASCR. He presented with low-grade fever and abdominal discomfort. He was evaluated with fluorodeoxyglucose positron emission tomography scan followed by omental biopsy that confirmed disease relapse. He received second-line therapy containing bortezomib and daratumumab and achieved remission (CR2). Subsequently, he underwent HDCT/ASCR. He has been clinically asymptomatic in good general condition having disease-free survival of 18 months after HDCT/ASCR. Our objective of presenting this case report is its complexity from presentation, diagnosis, and treatment. We take this opportunity to review the epidemiology and clinicopathological characteristics of PBL, as well as discuss the advancements in therapeutic options of this challenging disease.
Keywords
plasmablastic lymphoma - HIV infection - combined antiretroviral therapy - autologous stem cell transplant
Introduction
Plasmablastic lymphoma (PBL) is a variant of non-Hodgkin lymphoma with an aggressive biology. The management of this disease poses both diagnostic and therapeutic challenges in view of distinctive morphology, immunohistochemistry profile, and atypical clinical presentation along with the lack of standard treatment in the upfront and relapse settings. This leads to high rates of disease relapse and subsequent high mortality.[1] The prognosis remains poor due to early relapse and resistance to conventional cytotoxic agents from cyclophosphamide, doxorubicin, vincristine, and prednisolone (CHOP)-like regimen. There have been case reports where prolonged remission has been achieved with multiple myeloma-like treatment.[2] Retrospective analysis from large phase 2 trials, single-center experiences, and case reports have shown the benefit of high-dose chemotherapy with autologous stem cell rescue (HDCT/ASCR) in human immunodeficiency virus (HIV)-positive patients with relapsed non-Hodgkin lymphoma.[3] The prognosis of PBL in relapse setting is poor and there may be benefit of early HDCT/ASCR in the course of disease especially in high-risk subtypes. To achieve better outcome, we need to explore the role of HDCT/ASCR after achieving first remission (CR1) and in relapse setting in the case of HIV-positive patients with PBL.
Case Report
Our patient was diagnosed with HIV infection in 2012, followed by disseminated tuberculosis 2 years later that had presented as bilateral psoas muscle abscess. He was referred to us in 2016 with acute abdominal discomfort and oliguria. Computed tomographic (CT) scan revealed enlarged retroperitoneal lymph nodes causing bilateral ureteric compression (stage II). There was no history of B symptoms. Besides elevated lactate dehydrogenase (LDH) (750U/L), other blood investigations including complete blood count and renal function tests were normal. CT-guided biopsy of retroperitoneal lymph node was performed. With a strong suspicion of lymphoma, he was given intravenous dexamethasone after bone marrow biopsy. Following this, patient had symptomatic relief in abdominal discomfort and had resolution of oliguria within 8?hours. Histopathological examination reported PBL that also showed CD38+ and CD138+ and CD20- on immunohistochemistry. Epstein?Barr encoding region (EBER) in situ hybridization was not done. Cerebrospinal fluid (CSF) cytology for malignant cells was negative and bone marrow cytology testing was not involved. He received chemotherapy with B-EPOCH (bortezomib 1.3?mg/m2?intravenous push weekly, oral prednisolone 60?mg/m2?twice a day on days 1?5, etoposide 50?mg/m2, vincristine 0.4?mg/m2, and doxorubicin 10?mg/m2?as continuous infusion on days 1?4, with cyclophosphamide 750?mg/m2?on day 5) under pegylated G-CSF prophylaxis with intrathecal methotrexate. Fluorodeoxyglucose positron emission tomography (FDG PET/CT) scan after six cycles showed complete metabolic response. He continued antiretroviral (efavirenz, emtricitabine, tenofovir) and antitubercular therapy (levofloxacin, ethionamide, ethambutol). Follow-up FDG PET/CT scans were done annually for the following 2 years as our institutional practice to know the disease status that did not show any recurrence of disease.
In March 2019 (Disease Free Interval of 27 months), patient presented with low-grade fever and abdominal discomfort. Ultrasound of abdomen showed moderate ascites. Ascitic fluid analysis did not show atypical cells and Gene Xpert analysis for tuberculosis was negative. Real-time Ebstein?Barr virus by polymerase chain reaction of blood was negative. He had to undergo four sessions of large volume paracentesis over the next 2 weeks. Clinically, patient was in good performance status. There was no lymphadenopathy and he had doughy abdomen on palpation.
FDG PET/CT scan in March 2019 showed diffuse omental FDG uptake (SUVmax 4.2) with no evidence of nodal involvement (stage IIE) ([Fig. 1]). Laparoscopic omental biopsy was done in April 2019.
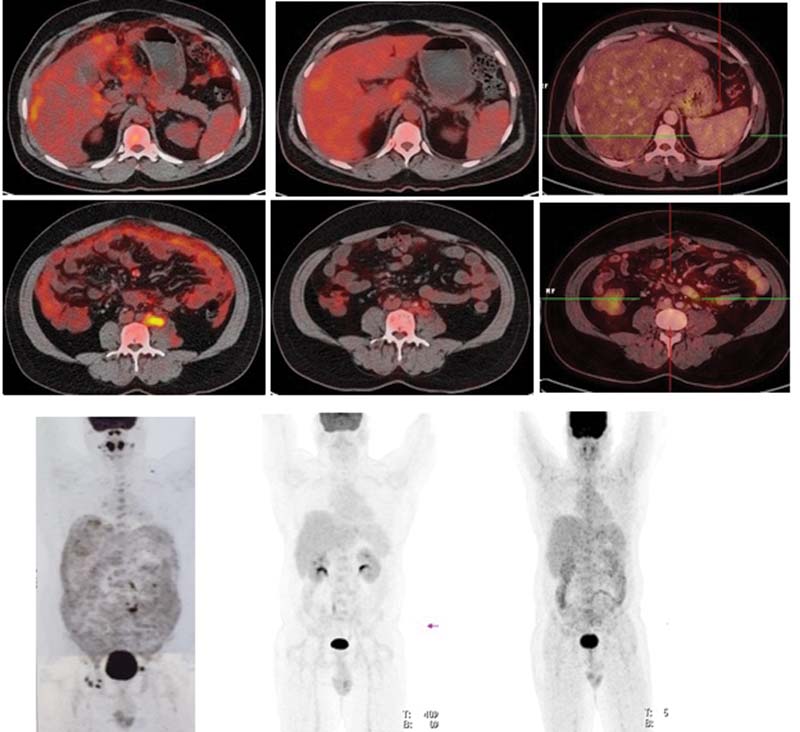
|?Fig. 1Fluorodeoxyglucose positron emission tomography fused images in March 2019 (left)?at the time of relapse, October 2019 (center)?after salvage chemotherapy and December 2020?13 months after transplant. Maximum intensity projection images in March 2019 (left)?at the time of relapse, October 2019 (center)?after salvage chemotherapy and December 2020?13 months after transplant.
Histopathological findings of hematoxylin and eosin stain ([Fig. 2A]) showed sheets of large atypical lymphoid cells with plasmacytic differentiation with abundant cytoplasm, paranuclear hof, and large nuclei with an immunoblastic appearance. IHC was positive for CD38 ([Fig. 2B]), CD138 ([Fig. 2C]), and negative for LCA, CD79a, CD20, CD3, pancytokeratin, and calretinin. EBER in situ hybridization was not done. With this, diagnosis of relapsed PBL was established.
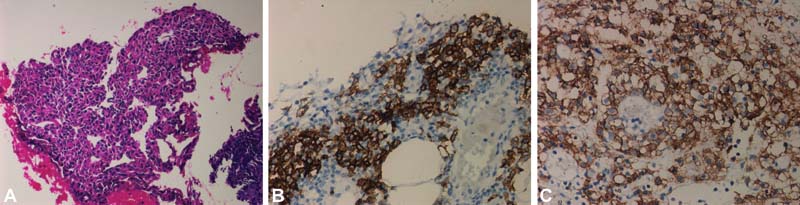
|?Fig. 2(A) Low power view showing sheets of plasmacytoid cells in omental fat. (B) Plasma cells showing strong membranous positivity with CD38. (C) Plasma cells showing strong membranous positivity with CD138.
After the confirmation of relapse, he received salvage chemotherapy with three cycles of 3 weekly ifosfamide, etoposide, and carboplatin along with weekly bortezomib, daratumumab, and dexamethasone (Vdd) for 9 weeks from May 2019 to July 2019. He tolerated this therapy well without any adverse events. There was clinical improvement with softening of abdomen and resolution of ascitic fluid on ultrasound examination after 3 weeks of starting chemotherapy.
FDG PET/CT scan 6 weeks after three cycles showed complete metabolic response ([Fig. 1]). There was a detailed discussion with patient and his immediate family members about long-term outcome, high risk of disease relapse, limited available treatment options, and the risks and benefits associated with HDCT/ASCR. He was also explained risk of transplant-related mortality and exacerbation of preexisting HIV infection and tuberculosis.
Baseline HIV viral load was negligible. CD4 count was 467cells/?L and TB Gold test was negative. Hematopoietic stem cells were mobilized with G-CSF 10 ?g/kg body weight from days 1 to 5 with injection plerixafor 0.24?mg/kg body weight on days 4 and 5. Two days of peripheral blood stem cell apheresis yielded CD34 cell count of 3.87???106?cells/kg body weight.
He was continued on combined antiretroviral therapy (cART) with abacavir, dolutegravir, and lamivudine combination once daily and this was continued as per the advice of infectious disease specialist. He was started on prophylactic ciprofloxacin, acyclovir, and fluconazole. He received myeloablative conditioning with lomustine, cytarabine, cyclophosphamide, etoposide regimen followed by stem cell infusion in November 2019. He required six units of irradiated packed RBC and three units of irradiated platelet concentrates during posttransplant hematopoietic recovery. Apart from grade 1 oral Mucositis, no other chemotherapy-related toxicities or adverse events were observed. He was engrafted on day +11 (granulocyte) and day +15 (platelet) and was subsequently discharged on day +18. HIV viral load (<20>
Patient has been on monthly follow-up with clinical examination and imaging. He is asymptomatic and has gained weight. His hemogram, liver, renal function tests, serum LDH in December 2020 are normal. PET CT scan in December 2020 ([Fig. 1]) showed no evidence of disease, translating into disease-free survival (DFS) of 13 months after the transplant.
Discussion
PBL was first shown to have an association with HIV and EBV coinfection and was recognized as an aggressive subset of lymphoma by the World Health Organization.[1] [4] However, its association with HIV-negative individuals, such as those having undergone past organ transplantation and allogeneic hematopoietic stem cell transplant and in few of them who are immunocompetent, has been described.[5]
Delecluse et al first described series of PBL cases in 1997, where features such as presence of HIV infection and presentation in oral cavity were associated with aggressive tumor biology and conferred poor response to conventional chemotherapy, leading to dismal outcome.[6] These tumors have a predilection to extramedullary sites, of which oral cavity has been predominant, followed by other sites like gastrointestinal tract, lung, sinus, testicles, and bone.[7] Our patient had retroperitoneal lymphadenopathy causing bilateral ureteric obstruction at the time of first presentation, while at relapse there was involvement of peritoneum and omentum presenting with refractory ascites.
PBL cells have immunoblastic morphology and display plasmacytic differentiation on immunophenotyping, with strong expression of biomarkers such as CD38, CD138, MUM1, BLIMP1, XBP1, MYC and variable expression of biomarkers such as CD45, CD79a, EMA, and CD30. There is generally no expression of B cell markers such as CD20 and PAX5. Autoimmune diseases, chronic inflammation, previous history of treatment for malignancies like lymphoma and acute leukemia, and elderly age have been reported as risk factors in HIV-negative patients for PBL by Lysa group.[8]
The diagnosis of PBL can be challenging, and depends upon history, clinical presentation, immunoblastic morphology, and the characteristic immunophenotypic pattern of CD20 negativity with positive markers of postgerminal center B-cells and plasma cells, such as CD138/syndecan with exclusion of other closely resembling conditions. The outcome of patients with PBL without active treatment is grim with a median overall survival (OS) of 3 and 4 months for HIV-positive and HIV-negative patients, respectively.[9] In contrast, PBL patients who are HIV positive and achieve complete remission after chemotherapy have a better outcome.[10]
The use of CHOP is considered inadequate therapy. Current guidelines recommend more intensive regimens like infusional etoposide, vincristine and doxorubicin with bolus cyclophosphamide and prednisone (EPOCH), cyclophosphamide, vincristine, doxorubicin, methotrexate alternating with ifosfamide, etoposide, and cytarabine (CODOX-M/IVAC), or hyperfractionated cyclophosphamide, vincristine, doxorubicin, and dexamethasone alternating with methotrexate and cytarabine (hyper-CVAD).[11] [12] [13] Few studies have identified a survival benefit of using EPOCH over CHOP in patients with HIV-associated lymphomas.[14]
Our patient was treated with six cycles of bortezomib and EPOCH with intrathecal methotrexate prophylaxis and achieved complete remission (CR1). Intrathecal prophylaxis is mandatory in the treatment of PBL, as it has high risk of central nervous system progression either during the treatment or at the time of relapse.[15] Two cases of spontaneous remission of PBL with antiretroviral therapy[16] and one patient with?MYC?rearrangement have been reported.[17] Nearly 30% of PBL express CD30 marker and therefore a response was seen to brentuximab vedotin in patients with CD30-expressing relapsed PBL.[18]
CD38 is a transmembrane receptor highly expressed on the surface of plasma cells and plasmablasts. Therefore, daratumumab (human IgG1k anti-CD38 monoclonal antibody) could be a possible part of treatment protocol.[19] [20] As some cases of PBL including EBV-positive and EBV-negative exhibit high expression of PD-1 and PD-L1, these patients may benefit from checkpoint inhibitors.[21]
HIV-associated PBL patients often have?MYC?translocation, and as bromodomain extraterminal (BET) inhibitor (JQ1) can induce cell cycle arrest by the inhibition of?MYC?transcription in preclinical studies, this will make BET inhibitors as a promising agent in these patients.[22]
Agents like tocilizumab (interleukin-6 [IL-6] receptor antagonist) and siltuximab (monoclonal antibody against IL-6) have shown clinical response, probably by starving IL-6, or by inducing apoptosis in the PBL-1 cell line.[23] Plasmablastic cell lines (PBL-1) can be targeted by inhibiting the PI3K/Akt/mTOR pathway as this is one of the major IL-6 signaling pathways occurring downstream of IL6?6R/GP130/JAK.[21] Other future possible therapies specific to EBV-directed agents are arginine butyrate, ganciclovir, and autologous EBV-specific CAR T cells with anti-CD30 properties.[24] [25]
Autologous stem cell transplantation has been performed in few case reports, in first remission (CR1) and also in relapse setting, under the cover of cART. The experience with HDCT/ASCT in the relapsed setting is rather limited, although some suggest that persistent complete remission can be achieved in chemotherapy-sensitive disease using conditioning regimes like carmustine, etoposide, cytarabine, and melphalan.[26] An Italian study (Italian Cooperative Group on AIDS and Tumors) on five patients of seropositive PBL resulted in complete remission and prolonged OS after HDCT/ASCR.[27] Case report from Moffitt cancer center in four non-HIV PBL patients who underwent autologous HSCT of which three patients were in CR and one patient was in PR. The patient who was in PR had DFS of 14 months, other 3 patients who had CR had DFS 2, 18, and 38.5 months, respectively.[28] Our patient achieved complete remission (CR2) with salvage therapy and underwent HDCT/ASCR.
AlloHSCT for PBL patients with HIV infection has several challenges, such as curative aspect of HIV status, drug interactions between antiretroviral drugs and transplant related medications, risk of opportunistic infection, high incidence of concomitant infections like viral hepatitis, effect of HIV on quantitative and qualitative function of T cell, bone marrow microenvironment, and cytokine milieu.[29] In 2009, Hamdani and Devine reported a case of PBL in CR2 with AlloHSCT using reduced intensity conditioning regimen from a matched unrelated donor.[30]
Patient has completed 19 months DFS from time of autologous stem cell rescue, leading an active life and is under close observation.
To the best of our knowledge, this is the first case report from India of an HIV-positive patient with PBL who underwent successful HDCT/ASCR under the cover of antiretroviral therapy.
Conclusion
Bortezomib containing regimen is effective in both newly diagnosed and relapsed PBL. HDCT/ASCR is a feasible option with better DFS in patients with chemo-sensitive HIV-associated non-Hodgkin lymphoma disease. In HIV-infected patients, cART should be initiated or optimized under the supervision of an infectious disease specialist with experience in the potential interactions between anticancer agents and cART. We suggest continuing cART during the entire treatment of PBL including HDCT/ASCR.
Conflict of Interest
None declared.
Ethics
The ethics committee approval for publication (ECC/ONCO/June/28, dated: 28/06/2021) was obtained from Jaslok Hospital and Research Centre institutional ethics committee.
References
- uze T, Painschab MS, Seguin R. et al.?Plasmablastic lymphoma in Malawi. Infect Agent Cancer 2018; 13: 22
- roccoli A, Nanni L, Stefoni V. et al.?A patient with plasmablastic lymphoma achieving long-term complete remission after thalidomide-dexamethasone induction and double autologous stem cell transplantation: a case report. BMC Cancer 2018; 18 (01) 645
- l-Malki MM, Castillo JJ, Sloan JM, Re A.?Hematopoietic cell transplantation for plasmablastic lymphoma: a review. Biol Blood Marrow Transplant 2014; 20 (12) 1877-1884
- rimm KE, O'Malley DP.?Aggressive B cell lymphomas in the 2017 revised WHO classification of tumors of hematopoietic and lymphoid tissues. Ann Diagn Pathol 2019; 38: 6-10
- astillo JJ, Winer ES, Stachurski D. et al.?HIV-negative plasmablastic lymphoma: not in the mouth. Clin Lymphoma Myeloma Leuk 2011; 11 (02) 185-189
- elecluse HJ, Anagnostopoulos I, Dallenbach F. et al.?Plasmablastic lymphomas of the oral cavity: a new entity associated with the human immunodeficiency virus infection. Blood 1997; 89 (04) 1413-1420
- chichman SA, McClure R, Schaefer RF, Mehta P.?HIV and plasmablastic lymphoma manifesting in sinus, testicles, and bones: a further expansion of the disease spectrum. Am J Hematol 2004; 77 (03) 291-295
- chernonog E, Faurie P, Coppo P. et al.?Clinical characteristics and prognostic factors of plasmablastic lymphoma patients: analysis of 135 patients from the LYSA group. Ann Oncol 2017; 28 (04) 843-848
- astillo JJ, Winer ES, Stachurski D. et al.?Clinical and pathological differences between human immunodeficiency virus-positive and human immunodeficiency virus-negative patients with plasmablastic lymphoma. Leuk Lymphoma 2010; 51 (11) 2047-2053
- Castillo JJ, Winer ES, Stachurski D. et al.?Prognostic factors in chemotherapy-treated patients with HIV-associated Plasmablastic lymphoma. Oncologist 2010; 15 (03) 293-299
- Zelenetz AD, Gordon LI, Wierda WG. et al.?Diffuse large B-cell lymphoma version 1.2016. J Natl Compr Canc Netw 2016; 14 (02) 196-231
- Cortes J, Thomas D, Rios A. et al.?Hyperfractionated cyclophosphamide, vincristine, doxorubicin, and dexamethasone and highly active antiretroviral therapy for patients with acquired immunodeficiency syndrome-related Burkitt lymphoma/leukemia. Cancer 2002; 94 (05) 1492-1499
- Patel K, Feng L, Oki Y. et al.?Plasmablastic lymphoma: 28 patient single institution experience. Blood 2013; 122 (21) 4310
- Barta SK, Lee JY, Kaplan LD, Noy A, Sparano JA.?Pooled analysis of AIDS malignancy consortium trials evaluating rituximab plus CHOP or infusional EPOCH chemotherapy in HIV-associated non-Hodgkin lymphoma. Cancer 2012; 118 (16) 3977-3983
- Castillo JJ, Bibas M, Miranda RN.?The biology and treatment of plasmablastic lymphoma. Blood 2015; 125 (15) 2323-2330
- Yordanova K, Stilgenbauer S, Bohle RM. et al.?Spontaneous regression of a plasmablastic lymphoma with MYC rearrangement. Br J Haematol 2019; 186 (06) e203-e207
- Montes-Moreno S, Martinez-Magunacelaya N, Zecchini-Barrese T. et al.?Plasmablastic lymphoma phenotype is determined by genetic alterations in MYC and PRDM1. Mod Pathol 2017; 30 (01) 85-94
- Holderness BM, Malhotra S, Levy NB, Danilov AV.?Brentuximab vedotin demonstrates activity in a patient with plasmablastic lymphoma arising from a background of chronic lymphocytic leukemia. J Clin Oncol 2013; 31 (12) e197-e199
- Palumbo A, Chanan-Khan A, Weisel K. et al; CASTOR Investigators.?Daratumumab, bortezomib, and dexamethasone for multiple myeloma. N Engl J Med 2016; 375 (08) 754-766
- Dimopoulos MA, Oriol A, Nahi H. et al; POLLUX Investigators.?Daratumumab, lenalidomide, and dexamethasone for multiple myeloma. N Engl J Med 2016; 375 (14) 1319-1331
- Laurent C, Fabiani B, Do C. et al.?Immune-checkpoint expression in Epstein-Barr virus positive and negative plasmablastic lymphoma: a clinical and pathological study in 82 patients. Haematologica 2016; 101 (08) 976-984
- Delmore JE, Issa GC, Lemieux ME. et al.?BET bromodomain inhibition as a therapeutic strategy to target c-Myc. Cell 2011; 146 (06) 904-917
- Mine S, Hishima T, Suganuma A. et al.?Interleukin-6-dependent growth in a newly established plasmablastic lymphoma cell line and its therapeutic targets. Sci Rep 2017; 7 (01) 10188
- Perrine SP, Hermine O, Small T. et al.?A phase 1/2 trial of arginine butyrate and ganciclovir in patients with Epstein-Barr virus-associated lymphoid malignancies. Blood 2007; 109 (06) 2571-2578
- Castillo JJ, Reagan JL, Bishop KD, Apor E.?Viral lymphomagenesis: from pathophysiology to the rationale for novel therapies. Br J Haematol 2014; 165 (03) 300-315
- Re A, Michieli M, Casari S. et al.?High-dose therapy and autologous peripheral blood stem cell transplantation as salvage treatment for AIDS-related lymphoma: long-term results of the Italian Cooperative Group on AIDS and Tumors (GICAT) study with analysis of prognostic factors. Blood 2009; 114 (07) 1306-1313
- Re A, Cattaneo C, Michieli M. et al.?High-dose therapy and autologous peripheral-blood stem-cell transplantation as salvage treatment for HIV-associated lymphoma in patients receiving highly active antiretroviral therapy. J Clin Oncol 2003; 21 (23) 4423-4427
- Liu JJ, Zhang L, Ayala E. et al.?Human immunodeficiency virus (HIV)-negative plasmablastic lymphoma: a single institutional experience and literature review. Leuk Res 2011; 35 (12) 1571-1577
- Holland HK, Saral R, Rossi JJ. et al.?Allogeneic bone marrow transplantation, zidovudine, and human immunodeficiency virus type 1 (HIV-1) infection. Studies in a patient with non-Hodgkin lymphoma. Ann Intern Med 1989; 111 (12) 973-981
- Hamadani M, Devine SM.?Reduced-intensity conditioning allogeneic stem cell transplantation in HIV patients with hematologic malignancies: yes, we can. Blood 2009; 114 (12) 2564-2566
Address for correspondence
Publication History
18 April 2022 (online)
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
|?Fig. 1Fluorodeoxyglucose positron emission tomography fused images in March 2019 (left)?at the time of relapse, October 2019 (center)?after salvage chemotherapy and December 2020?13 months after transplant. Maximum intensity projection images in March 2019 (left)?at the time of relapse, October 2019 (center)?after salvage chemotherapy and December 2020?13 months after transplant.
|?Fig. 2(A) Low power view showing sheets of plasmacytoid cells in omental fat. (B) Plasma cells showing strong membranous positivity with CD38. (C) Plasma cells showing strong membranous positivity with CD138.
References
- chab MS, Seguin R. et al.?Plasmablastic lymphoma in Malawi. Infect Agent Cancer 2018; 13: 22
- roccoli A, Nanni L, Stefoni V. et al.?A patient with plasmablastic lymphoma achieving long-term complete remission after thalidomide-dexamethasone induction and double autologous stem cell transplantation: a case report. BMC Cancer 2018; 18 (01) 645
- l-Malki MM, Castillo JJ, Sloan JM, Re A.?Hematopoietic cell transplantation for plasmablastic lymphoma: a review. Biol Blood Marrow Transplant 2014; 20 (12) 1877-1884
- rimm KE, O'Malley DP.?Aggressive B cell lymphomas in the 2017 revised WHO classification of tumors of hematopoietic and lymphoid tissues. Ann Diagn Pathol 2019; 38: 6-10
- astillo JJ, Winer ES, Stachurski D. et al.?HIV-negative plasmablastic lymphoma: not in the mouth. Clin Lymphoma Myeloma Leuk 2011; 11 (02) 185-189
- elecluse HJ, Anagnostopoulos I, Dallenbach F. et al.?Plasmablastic lymphomas of the oral cavity: a new entity associated with the human immunodeficiency virus infection. Blood 1997; 89 (04) 1413-1420
- chichman SA, McClure R, Schaefer RF, Mehta P.?HIV and plasmablastic lymphoma manifesting in sinus, testicles, and bones: a further expansion of the disease spectrum. Am J Hematol 2004; 77 (03) 291-295
- chernonog E, Faurie P, Coppo P. et al.?Clinical characteristics and prognostic factors of plasmablastic lymphoma patients: analysis of 135 patients from the LYSA group. Ann Oncol 2017; 28 (04) 843-848
- astillo JJ, Winer ES, Stachurski D. et al.?Clinical and pathological differences between human immunodeficiency virus-positive and human immunodeficiency virus-negative patients with plasmablastic lymphoma. Leuk Lymphoma 2010; 51 (11) 2047-2053
- Castillo JJ, Winer ES, Stachurski D. et al.?Prognostic factors in chemotherapy-treated patients with HIV-associated Plasmablastic lymphoma. Oncologist 2010; 15 (03) 293-299
- Zelenetz AD, Gordon LI, Wierda WG. et al.?Diffuse large B-cell lymphoma version 1.2016. J Natl Compr Canc Netw 2016; 14 (02) 196-231
- Cortes J, Thomas D, Rios A. et al.?Hyperfractionated cyclophosphamide, vincristine, doxorubicin, and dexamethasone and highly active antiretroviral therapy for patients with acquired immunodeficiency syndrome-related Burkitt lymphoma/leukemia. Cancer 2002; 94 (05) 1492-1499
- Patel K, Feng L, Oki Y. et al.?Plasmablastic lymphoma: 28 patient single institution experience. Blood 2013; 122 (21) 4310
- Barta SK, Lee JY, Kaplan LD, Noy A, Sparano JA.?Pooled analysis of AIDS malignancy consortium trials evaluating rituximab plus CHOP or infusional EPOCH chemotherapy in HIV-associated non-Hodgkin lymphoma. Cancer 2012; 118 (16) 3977-3983
- Castillo JJ, Bibas M, Miranda RN.?The biology and treatment of plasmablastic lymphoma. Blood 2015; 125 (15) 2323-2330
- Yordanova K, Stilgenbauer S, Bohle RM. et al.?Spontaneous regression of a plasmablastic lymphoma with MYC rearrangement. Br J Haematol 2019; 186 (06) e203-e207
- Montes-Moreno S, Martinez-Magunacelaya N, Zecchini-Barrese T. et al.?Plasmablastic lymphoma phenotype is determined by genetic alterations in MYC and PRDM1. Mod Pathol 2017; 30 (01) 85-94
- Holderness BM, Malhotra S, Levy NB, Danilov AV.?Brentuximab vedotin demonstrates activity in a patient with plasmablastic lymphoma arising from a background of chronic lymphocytic leukemia. J Clin Oncol 2013; 31 (12) e197-e199
- Palumbo A, Chanan-Khan A, Weisel K. et al; CASTOR Investigators.?Daratumumab, bortezomib, and dexamethasone for multiple myeloma. N Engl J Med 2016; 375 (08) 754-766
- Dimopoulos MA, Oriol A, Nahi H. et al; POLLUX Investigators.?Daratumumab, lenalidomide, and dexamethasone for multiple myeloma. N Engl J Med 2016; 375 (14) 1319-1331
- Laurent C, Fabiani B, Do C. et al.?Immune-checkpoint expression in Epstein-Barr virus positive and negative plasmablastic lymphoma: a clinical and pathological study in 82 patients. Haematologica 2016; 101 (08) 976-984
- Delmore JE, Issa GC, Lemieux ME. et al.?BET bromodomain inhibition as a therapeutic strategy to target c-Myc. Cell 2011; 146 (06) 904-917
- Mine S, Hishima T, Suganuma A. et al.?Interleukin-6-dependent growth in a newly established plasmablastic lymphoma cell line and its therapeutic targets. Sci Rep 2017; 7 (01) 10188
- Perrine SP, Hermine O, Small T. et al.?A phase 1/2 trial of arginine butyrate and ganciclovir in patients with Epstein-Barr virus-associated lymphoid malignancies. Blood 2007; 109 (06) 2571-2578
- Castillo JJ, Reagan JL, Bishop KD, Apor E.?Viral lymphomagenesis: from pathophysiology to the rationale for novel therapies. Br J Haematol 2014; 165 (03) 300-315
- Re A, Michieli M, Casari S. et al.?High-dose therapy and autologous peripheral blood stem cell transplantation as salvage treatment for AIDS-related lymphoma: long-term results of the Italian Cooperative Group on AIDS and Tumors (GICAT) study with analysis of prognostic factors. Blood 2009; 114 (07) 1306-1313
- Re A, Cattaneo C, Michieli M. et al.?High-dose therapy and autologous peripheral-blood stem-cell transplantation as salvage treatment for HIV-associated lymphoma in patients receiving highly active antiretroviral therapy. J Clin Oncol 2003; 21 (23) 4423-4427
- Liu JJ, Zhang L, Ayala E. et al.?Human immunodeficiency virus (HIV)-negative plasmablastic lymphoma: a single institutional experience and literature review. Leuk Res 2011; 35 (12) 1571-1577
- Holland HK, Saral R, Rossi JJ. et al.?Allogeneic bone marrow transplantation, zidovudine, and human immunodeficiency virus type 1 (HIV-1) infection. Studies in a patient with non-Hodgkin lymphoma. Ann Intern Med 1989; 111 (12) 973-981
- Hamadani M, Devine SM.?Reduced-intensity conditioning allogeneic stem cell transplantation in HIV patients with hematologic malignancies: yes, we can. Blood 2009; 114 (12) 2564-2566