 PDF
PDF  Views
Views  Share
Share


Rhabdoid Meningioma of Brain - A Rare Aggressive Tumor
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2017; 38(02): 218-219
DOI: DOI: 10.4103/ijmpo.ijmpo_87_16
Abstract
Rhabdoid meningioma is a rare aggressive variant of meningioma, regarded as WHO Grade III type. Histologically and cytologically, it is distinctive type having abundant eosinophilic cytoplasm, cytoplasmic inclusion with eccentrically placed vesicular nuclei and prominent nucleoli. High recurrence rate and poor outcome are important features. Here, we are presenting a rare case of rhabdoid meningioma found in a recurrent meningioma of the posterior fossa in a middle-aged female. We emphasized the squash cytology and histology finding of the rare neoplasm.
Publication History
Article published online:
06 July 2021
© 2017. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Abstract
Rhabdoid meningioma is a rare aggressive variant of meningioma, regarded as WHO Grade III type. Histologically and cytologically, it is distinctive type having abundant eosinophilic cytoplasm, cytoplasmic inclusion with eccentrically placed vesicular nuclei and prominent nucleoli. High recurrence rate and poor outcome are important features. Here, we are presenting a rare case of rhabdoid meningioma found in a recurrent meningioma of the posterior fossa in a middle-aged female. We emphasized the squash cytology and histology finding of the rare neoplasm.
Introduction
Meningiomas are slow-growing central nervous system (CNS) neoplasm of meningothelial origin. However, some of the meningiomas have aggressive behavior (WHO Grade II: atypical, clear cell and choroid and WHO Grade III-papillary and anaplastic variant).[1] Rhabdoid meningiomas are rare aggressive variant, adopted in WHO classification of CNS neoplasm (2000) and belonged to WHO Grade III subtype.[1,2] This tumor is associated with rapid growth, high incidence of recurrence, and poor survival than others.[1,2] Here, we are reporting a rare case of rhabdoid meningioma in a middle-aged male patient with an emphasis on squash cytology and histology.
Case Report
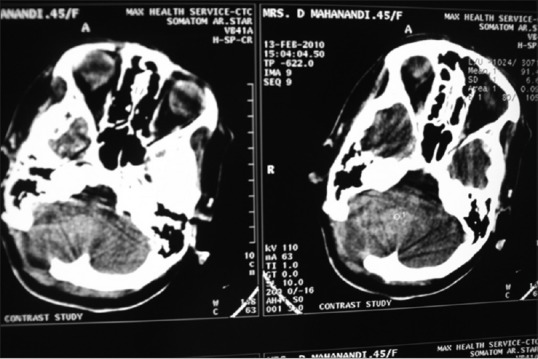
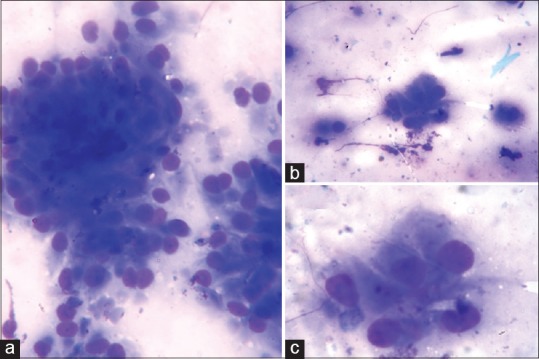
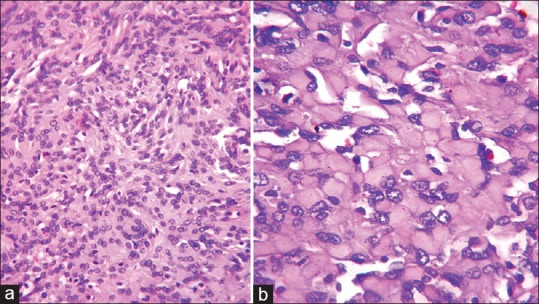
A 45-year-old female presented with headache, vertigo, and vomiting for the last 2 days and altered sensorium for the last 1 h. She had a past history of posterior fossa tumor and was operated 1 year back. Histologically, it was diagnosed as meningothelial meningioma of posterior fossa (WHO Grade I). Her hematological and biochemical tests were within normal limits except mild anemia. Electrolyte assay showed mild hyponatremia (Na-129 mmol/l). Computed tomography scan revealed a brightly contrast-enhancing dural-based mass at previously operated location [Figure 1]. Clinical and radiological diagnosis was recurrent meningioma. Her visual acuity was normal, but both the fundus showed papilledema. She had undergone repeat surgery, and intraoperative squash cytology was taken. The squash cytology revealed monotonous meningothelial cells arranged in lobules [Figure 2a]. There were some meningothelial cells with characteristic abundant cytoplasm and round nuclei pushing to periphery (rhabdoid cells) [Figure [Figure2b2b and andc].c]. In gross examination, the resected tumor was a grayish mass 5.5 cm × 4 cm × 3 cm. In histopathology, microscopy revealed a solid mass composed of meningothelial cells in sheets and in whorled pattern [Figure 3a]. There are areas of monomorphous sheets of cells with abundant eosinophilic cytoplasm with eccentrically placed vesicular nuclei and prominent nucleoli [Figure 3b]. The cells contained spherical masses of eosinophilic inclusions pushing the nuclei to the periphery. Areas of necrosis and psammoma bodies are also found. Mitotic count was 4–8/10 high power field. Final histopathological diagnosis was rhabdoid meningioma.
| Figure 1:Chest radiograph shows well-circumscribed mass in mediastinum
| Figure 2:Computed tomography thorax shows well-circumscribed mass in mediastinum
| Figure 3:Microscopic changes of mature teratoma [Low power]
Discussion
Rhabdoid meningioma is a very rare aggressive variant of meningioma.[2] Most of the meningiomas are among Grade I (WHO).[2,3] Only 5%–7% meningioma are atypical (Grade II) and 3% are anaplastic type (WHO Grade III).[2] Rhabdoid transformation of the meningothelial tumor was first described by Perry et al. in 1998.[3,4] It was included in WHO classification 2000 as a subtype of meningioma with high risk of recurrence.[3] Although cases have been reported of different age, most of the cases occur in young and middle age with an equal incidence in male and female.[1,3,5] The term rhabdoid refers to the resemblance of neoplastic cells to rhabdomyoblast without true skeletal muscle differentiation.[1] Ultrastructurally, it represents whorls of intermediate filaments expressing vimentin and occasionally cytokeratin.[6] Tumor with rhabdoid morphology was initially introduced in renal neoplasm with aggressive behavior.[6] Rhabdoid morphology has been identified in different tumors such as carcinomas, sarcomas, gliomas, and melanoma.[1]
Histologically, the rhabdoid morphology cells have large round to oval with abundant eosinophilic cytoplasm, eccentrically placed nuclei with prominent nuclei.[3] Paranuclear cytoplasmic eosinophilic inclusions are frequently found.[3] Most of the cases exhibit rhabdoid morphology with histological evidence of meningothelial differentiation.[3] In our case also, the tumor exhibited typical meningothelial differentiation with areas of rhabdoid morphology. Infiltrating growth and focal necrosis are also associated features and were evident in our case. Differential diagnoses of rhabdoid meningioma include atypical teratoid/rhabdoid tumor, metastatic carcinoma, melanoma, sarcoma, and mega cell medulloblastoma.[1,3,5] Histological diagnosis depends on the evidence of meningothelial differentiation (whorls, nuclear characters, eosinophilic inclusion bodies) and immunohistochemistry findings (epithelial membrane antigen, vimentin, and progesterone receptor positive).[1]
Recurrence rate is very high approaching about 87%.[5] In our case, it was a recurrent tumor after 18 months of surgery. Radical surgery and postoperative radiotherapy of 60 GY (conventional fractional) are the therapeutic modality of choice.[1] However, stereotactic radiosurgery, preoperative chemoembolization, and combined radio-chemotherapy are the other optional modalities.[2] Median survival is <3 href="https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5582564/#ref2" rid="ref2" class=" bibr popnode" role="button" aria-expanded="false" aria-haspopup="true" xss=removed>2]
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Kar A, Rath G, Mohanty L, Behera P, Mohapatro S, Lenka A et al. Rhabdoid meningioma-An uncommon and aggressive variant. J Cancer Sci Ther 2013;5:343-5.
- Kakar V, Elsmore A. Rhabdoid meningioma: Rare and highly aggressive. Internet J Neurosurg 2005;3:1-5.
- Matyja E, Grajkowska W, Nauman P, Bonicki W, Bojarski P, Marchel A. Necrotic rhabdoid meningiomas with aggressive clinical behavior. Clin Neuropathol 2010;29:307-16.
- Perry A, Scheithauer BW, Stafford SL, Abell-Aleff PC, Meyer FB. “Rhabdoid” meningioma: An aggressive variant. Am J Surg Pathol 1998;22:1482-90.
- Han H, Du P, Zhang Y, Deng Y. Diagnosis and differential diagnosis of rhabdoid meningioma: One case report and literature review. Clin Oncol Cancer Res 2009;6:303-6.
- Jansen JC, Turner J, Sheehy J, Fagan PA. Recurrent rhabdoid meningioma: Case report. Skull Base 2003;13:51-4.
| Figure 1:Chest radiograph shows well-circumscribed mass in mediastinum
| Figure 2:Computed tomography thorax shows well-circumscribed mass in mediastinum
| Figure 3:Microscopic changes of mature teratoma [Low power]
References
- Kar A, Rath G, Mohanty L, Behera P, Mohapatro S, Lenka A et al. Rhabdoid meningioma-An uncommon and aggressive variant. J Cancer Sci Ther 2013;5:343-5.
- Kakar V, Elsmore A. Rhabdoid meningioma: Rare and highly aggressive. Internet J Neurosurg 2005;3:1-5.
- Matyja E, Grajkowska W, Nauman P, Bonicki W, Bojarski P, Marchel A. Necrotic rhabdoid meningiomas with aggressive clinical behavior. Clin Neuropathol 2010;29:307-16.
- Perry A, Scheithauer BW, Stafford SL, Abell-Aleff PC, Meyer FB. “Rhabdoid” meningioma: An aggressive variant. Am J Surg Pathol 1998;22:1482-90.
- Han H, Du P, Zhang Y, Deng Y. Diagnosis and differential diagnosis of rhabdoid meningioma: One case report and literature review. Clin Oncol Cancer Res 2009;6:303-6.
- Jansen JC, Turner J, Sheehy J, Fagan PA. Recurrent rhabdoid meningioma: Case report. Skull Base 2003;13:51-4.