 PDF
PDF  Views
Views  Share
Share


Role of triple test score in the evaluation of palpable breast lump
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2015; 36(02): 123-127
DOI: DOI: 10.4103/0971-5851.158846
Abstract
Introduction: Fine-needle aspiration cytology (FNAC) method is safe, reliable and time saving outdoor procedure with little discomfort to the patient for detecting Carcinoma breast. The efficacy can further be enhanced when physical breast examination, mammography and FNAC (the triple test [TT]) are jointly taken into consideration. Aims and Objectives : The aim was to evaluate the role of TT score (TTS) in palpable breast masses. Materials and Methods: This prospective study was carried out from May 2010 to April 2012. In the subjects referred to the Department of Pathology for FNAC of the breast mass, the TTS was calculated, and histopathological findings were noted. Results: In the study period TTS score was calculated in 200 cases out of 225 FNAC′s of breast. Of 124 benign cases on cytology, only three showed discordant TTS. Out of 62 malignant cases, 61 showed concordant TTS and one case of mastitis on histopathology showed TTS of five. Out of all the benign lesions, two cases of fibrocystic disease and a single case of phylloides tumor gave a TTS ≥6. These cases were diagnosed as infiltrating ductal carcinoma and angiosarcoma respectively on histopathology. Histopathological correlation was possible in only 70 patients. Of these 70, 28 were from the benign category and 42 were from the malignant category. TTS of ≥6 has a sensitivity of 97.44%, specificity of 100%. FNAC has a sensitivity of 88.37%, specificity of 96.42%. Conclusions: TT reliably guides evaluation of palpable breast masses. Histological correlation indicated TTS to be better diagnostic tool than FNAC alone.
Publication History
Article published online:
12 July 2021
© 2015. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Abstract
Introduction:
Fine-needle aspiration cytology (FNAC) method is safe, reliable and time saving outdoor procedure with little discomfort to the patient for detecting Carcinoma breast. The efficacy can further be enhanced when physical breast examination, mammography and FNAC (the triple test [TT]) are jointly taken into consideration.
Aims and Objectives:
The aim was to evaluate the role of TT score (TTS) in palpable breast masses.
Materials and Methods:
This prospective study was carried out from May 2010 to April 2012. In the subjects referred to the Department of Pathology for FNAC of the breast mass, the TTS was calculated, and histopathological findings were noted.
Results:
In the study period TTS score was calculated in 200 cases out of 225 FNAC's of breast. Of 124 benign cases on cytology, only three showed discordant TTS. Out of 62 malignant cases, 61 showed concordant TTS and one case of mastitis on histopathology showed TTS of five. Out of all the benign lesions, two cases of fibrocystic disease and a single case of phylloides tumor gave a TTS ≥6. These cases were diagnosed as infiltrating ductal carcinoma and angiosarcoma respectively on histopathology. Histopathological correlation was possible in only 70 patients. Of these 70, 28 were from the benign category and 42 were from the malignant category. TTS of ≥6 has a sensitivity of 97.44%, specificity of 100%. FNAC has a sensitivity of 88.37%, specificity of 96.42%.
Conclusions:
TT reliably guides evaluation of palpable breast masses. Histological correlation indicated TTS to be better diagnostic tool than FNAC alone.
INTRODUCTION
Despite breathtaking advances in science and technology, breast cancer still remains mankind's one of the most dreaded maladies.[1] Timely diagnosis and well planned, and executed treatment strategy are the cornerstones of successful management of this entity.[2]
Self-breast examination or a Clinical breast examination alone may not be sufficient in identifying potentially malignant breast lesions. On such occasions X-ray mammography or Sonomammography can demonstrate such lesions, which can then be subjected to fine needle aspiration cytology (FNAC) for pathological confirmation as FNAC has stood the test of time as a safe, reliable and time saving outdoor procedure with little discomfort to the patient.[3]
X-ray mammographic screening was introduced as a means to detect small, nonpalpable, asymptomatic breast carcinomas. Principal X-ray mammographic signs of breast carcinoma are densities and calcifications. In about 10% of cases, carcinomas are missed by mammography. The principal causes of these failures are the presence of surrounding radio dense tissue that obscures the tumor, the absence of calcification, small size, diffuse infiltrative pattern with little or no desmoplastic response, or a location close to chest wall or in periphery of breast. Sonomammography distinguishes between solid and cystic lesions and can define more precisely the borders of solid lesions. Most palpable masses that are not imaged at all by mammography are detectable by ultrasound.[4]
While traditional diagnostic approach to palpable breast masses mostly involved direct FNAC of the referred case without much attention to the clinical or mammography diagnosis, the possibility that the diagnostic efficacy could further be enhanced when physical breast examination, mammography and FNAC (the triple test [TT]) are jointly taken into consideration as reported in other studies.[5,6,7,8]
Various studies have found nearly 100% diagnostic accuracy of the TT for palpable breast masses when all three elements (i.e., physical examination, mammogram and FNAC) are concordant. A clinician can proceed directly with definitive therapy without an interventional open biopsy if all the components of TT are malignant. If all the components are found to be benign, the patient can then be safely observed.[5,6,7,8]
In September, 1996, National Cancer Institute sponsored conference was held for the purpose of defining a uniform approach to breast fine needle aspiration (FNA) biopsy, and to address some of the controversies related to breast FNA, including the use of core biopsies. The conference recommendations acknowledged the value of the “TT,” that is, the combination of physical examination, imaging findings, and cytological examination in the reliable diagnosis of breast cancer. Consequently, it was suggested that a recommendation be included in the cytopathology reports of breast FNAs to support the clinical application of the “TT.”[9]
Considering these facts the current study was carried out with an aim of evaluating the role of TT score (TTS) in palpable breast masses by calculating the TTS in FNAC cases; classifying in to benign, malignant and nonconcordant cases according to TTS, correlation with histopathology and finding the effectiveness of TTS in comparison to FNAC alone.
MATERIALS AND METHODS
This prospective study was carried out from May 2010 to April 2012. The subjects concerned included all the female patients, which were referred to the Department of Pathology for FNAC of the breast mass.
Females having palpable breast lump and voluntary consent were included in the study. Patients with hemorrhagic diathesis, breast mass associated with pregnancy, associated localized skin infection and patients on oral anticoagulants were excluded.
The entire procedure was explained to the patient. Complete clinical history along with mammographic/sonomammographic findings was noted. Physical examination of the breast mass by palpation was done. Finally, the FNAC was done. Air dried smears were fixed and stained with May Grunwald Giemsa technique. One smear was fixed with 95% alcohol for a period of 30 min before drying. Staining was carried out on the alcohol fixed slides by Papanicolaou stain. FNAC findings were noted down. Lesion was classified in to inadequate, benign, atypical, suspicious, and malignant.
The TTS was calculated.[5,6,7,8] It included three main diagnostic features of the procedure namely physical examination, mammography and FNAC. Each component of TT was assigned 1, 2 or 3 points for a benign, suspicious or malignant result respectively. TTS is the sum of these scores. TTS has a minimum score of 3 (concordant benign) and a maximum score of 9 (concordant malignant). All lesions with TTS ≤4 are considered benign; all lesions with TTS ≥6 are considered malignant. The patients were followed-up for mastectomy or biopsy. Histopathological findings were noted. The statistical analyses were done to find the ability of TTS and FNAC to detect the presence of malignancy in the breast in comparison to histopathology. For this sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV) and accuracy/efficiency were calculated.
RESULTS
In the study period of the present study from May 2010 to April 2012, 225 FNAC's of breasts were done. TTS score was calculated in 200 cases.
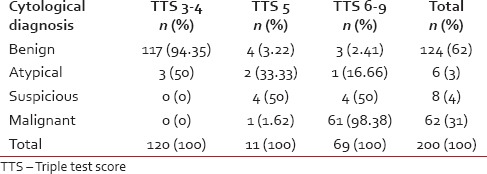
Table 1 shows the TTS applied to the spectrum of lesions on cytology. TTS was available for 200 cases. Of the 124 benign lesions on cytology, a TTS score of 3-4 was seen in 117 cases, Out of the total 62 cases labeled as malignant, 61 cases had a TTS score of ≥6.
Table 1
Triple test score in spectrum of lesions on cytology
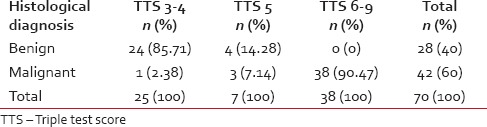
The Table 2 correlates TTS with Histopathology. In the present study though TT was applied to 200 odd cases, its impact could be evaluated in 70 out of 200 as histopathological correlation was possible in only 70 patients. Out of these 70, 28 were from the benign category and 42 were from the malignant category. In the present study, out of the 28 benign cases 24 cases had the TTS of 3-4 and only four had a TTS of 5. Out of the 42 malignant cases, 38 cases had the TTS of ≥6, three had a TTS of 5 and only one had a TTS of 3-4.
Table 2
Correlation of TTS with histopathology
The correlation of the benign histopathological lesions with the TTS pointed that out of the 12 cases of fibroadenoma, 11 cases (91.66%) had the TTS of 3-4 and only 1 (8.33%) had a TTS of 5. All 9 cases of fibrocystic disease that had a TTS showed it to be 3-4. Single case of duct ectasia and atrophic breast tissue showed a TTS of 5 each. Out of 5 cases of mastitis, four had TTS of 3-4 and one case had TTS of 5.
The correlation of the malignant histopathological lesions with the TTS as seen in present study shows that out of the 35 cases of infiltrating ductal carcinoma (IDC) that had a TTS, 31 cases (88.57%) had the TTS of ≥6, 3 (8.57%) had a TTS of 5 and only 1 (2.85%) had a TTS of 3-4. Both cases of lobular carcinoma, and single case of lymphoma, medullary carcinoma, angiosarcoma and mucinous carcinoma showed a TTS of ≥6 each.
The Statistical analyses showed that a TTS was 100% sensitive and 97.43% specific in diagnosing benign lesions. It had a PPV of 96% and a NPV of 97.44% in diagnosing benign lesions. Similarly, a TTS was 97.44% sensitive and 100% specific in diagnosing malignant lesions. Furthermore, it had PPV of 100% and a NPV of 96% in diagnosing malignant lesion. In the present study, TTS had an accuracy/efficiency of 98.41%.
The Statistical Analyses of FNAC as a diagnostic test to detect the presence of malignancy in the breast was done. FNAC was 88.37% sensitive and 96.42% specific in diagnosing malignant lesions. Also, FNAC had PPV of 97.43% and a NPV of 84.37% in diagnosing malignant lesion. In the present study, it had an accuracy/efficiency of 91.54%.
DISCUSSION
The “TT,” was initially described in the mid-1970s, by Johansen C. as the evaluation of palpable breast masses by physical examination, mammography, and FNAC. The TT has proved a reliable tool for the accurate diagnosis of palpable breast masses, due to its technical simplicity, and resulted in substantially reduced expense and morbidity compared with open surgical biopsy.[5]
Due to the reduced sensitivity and specificity of lesion detection by mammography in young women under 40 and the usefulness of sonography in this group of patients, researchers dealing with women under 40 combined sonography with mammography to the scoring system and the modified TTS was introduced which is an integration of clinical breast examination, sonography and FNA.[10]
The TTS reliably guides evaluation and treatment of breast lesions. Lesions scoring 3 or 4 are always benign. Lesions with scores ≥6 are malignant and should be treated accordingly. Confirmatory biopsy is required only for the lesions that receive a TTS of 5.[11]
In the present study, three cytological benign cases were indicated as malignant by TTS. All three were confirmed malignant on biopsy. Hence, clinical and mammography findings may be important in some cases. Proper area might not have been aspirated in these discordant cases. TTS of 5 indicates suspicious lesions, and they are to be evaluated by biopsy. All malignant cases on cytology showed TTS of ≥6, except one case where TTS was 5. So, malignant cases generally are not missed by TTS.
Two cases of fibrocystic disease and one case of phylloides tumor showed TTS ≥6. This indicates discordance and is possibly due to differences in appearance of different parts of the lesion on different modalities. As per present study, all cytological malignant cases showed TTS ≥6, except one case of IDC, where TTS was 5.
Histological correlation with TTS showed that in the present study, out of 28 histological benign cases 24 (85.71%) had concordant TTS (3-4) which correlates with studies by Ghafouri et al.[10] 84 (94.38%), Morris et al.[5] 152 (92.12%) and Hermansen et al.[12] 231 (73.80%). None of the benign cases in the present study showed discordant TTS which correlates with studies by Morris et al.[5] and Hermansen et al.;[12] but the study by Ghafouri et al.[10] showed 2 (2.24%) discordant cases with a TTS of ≥6. In the present study, 4 cases (14.28%) had a TTS of 5, which correlates with Ghafouri et al.[10] 3 (3.37%), Morris et al.[5] 13 (7.87%) and Hermansen et al.[12] 82 (26.19%). Present study suggests that TTS is a very good and reliable tool for diagnosis of fibrocystic disease. Fibroadenoma, mastitis and duct ectasia can give TTS of 5, if atypical cells are seen or clinical examination/mammography suggests suspicious lesions.
Table 3 indicates various studies showing TTS in malignant lesions on histopathology. In the present study, one histological malignant case had discordant TTS (3-4) which is in contrast to other studies who had no case in the TTS of 3-4. The only discordant case was benign cytologically, may be because of the sampling error of the sample, not from the representative area. These results suggest that TTS is a reliable tool for diagnosis of malignant lesions - IDC and its variants as well as tumors like angiosarcoma and lymphoma.
Table 3
Comparison of TTS in malignant lesions on histopathology
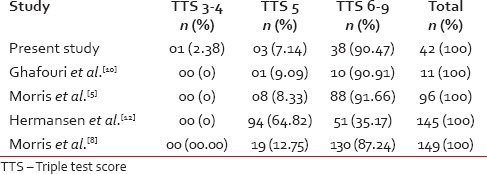
Table 4 indicates statistical analysis of TTS as a diagnostic tool in various studies. Hence, overall TTS has good sensitivity, specificity, PPV and NPV. Table 5 shows statistical analyses of FNAC as a diagnostic Test in various studies and indicates good sensitivity, specificity, PPV and NPV.
Table 4
Statistical analyses of TTS as a diagnostic tool in various studies
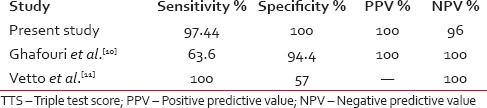
Table 5
Statistical analyses of FNAC as a diagnostic test in various studies
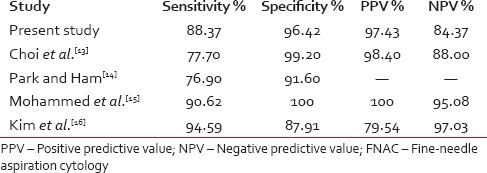
Although histological correlation has indicated FNAC to be a good diagnostic tool,[17] statistical analysis in the present study also indicates TTS to be a better tool than FNAC alone.
CONCLUSIONS
Triple test reliably guides evaluation of palpable breast masses. Benign breast lesions are common than malignant lesions, fibroadenoma and fibrocystic disease are more common in benign disease, whereas IDC accounts for the highest number of malignant lesions. Histological correlation indicated TTS to be better diagnostic tool than FNAC alone.
ACKNOWLEDGMENTS
Dr. Gandge S.G and Dr. Kachewar S.G, Department of Radiology, Dr. Baviskar P.K., Department of Surgery, Dr. Singh K. K., Department of Oncology, RMC, PIMS (DU), Loni.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.