 PDF
PDF  Views
Views  Share
Share


Ruptured Malignant Ovarian Tumor in an Adolescent Girl: A Rare Case Report
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2017; 38(02): 212-214
DOI: DOI: 10.4103/ijmpo.ijmpo_2_17
Abstract
Germ cell tumors which arise mainly in pediatric and adolescent age group, account for 30% of all ovarian tumors, but constitute only 5% of all malignant ovarian tumors. The presentation is usually insidious with the patient presenting with abdominal swelling and dull aching pain. We report a rare case of a malignant germ cell tumor in a 12-year-old girl who presented with acute abdomen due to spontaneous rupture of tumor resulting in hemoperitoneum. The patient was taken up for emergency laparotomy and left salpingo-opherectomy with omentectomy and drainage of hemoperitoneum was done. The authors conclude that ruptured malignant ovarian tumor should be considered in the differential diagnosis of any young girl presenting with abdominal mass and acute abdominal pain.
Publication History
Article published online:
06 July 2021
© 2017. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Abstract
Germ cell tumors which arise mainly in pediatric and adolescent age group, account for 30% of all ovarian tumors, but constitute only 5% of all malignant ovarian tumors. The presentation is usually insidious with the patient presenting with abdominal swelling and dull aching pain. We report a rare case of a malignant germ cell tumor in a 12-year-old girl who presented with acute abdomen due to spontaneous rupture of tumor resulting in hemoperitoneum. The patient was taken up for emergency laparotomy and left salpingo-opherectomy with omentectomy and drainage of hemoperitoneum was done. The authors conclude that ruptured malignant ovarian tumor should be considered in the differential diagnosis of any young girl presenting with abdominal mass and acute abdominal pain.
Introduction
Germ cell tumors which arise mainly in pediatric and adolescent age group account for 30% of all ovarian tumors but constitute only 5% of all malignant ovarian tumors.[1] The median age is 18 years. About 1/3 of the patients are premenarchal at the time of initial presentation.[2,3] Most granular cell tumors (GCTs) are often asymptomatic until they reach a very large size with compression of the neighboring structures. The usual presentation is lower abdominal pain and an abdominal mass. Only few cases present as acute abdomen due to torsion, infarction, or spontaneous rupture of the mass. The majority of GCTs have a good prognosis with surgery and chemotherapy, and patients may have a disease-free survival rate of over 80% in all stages.[4]
Case Report
A 12-year-old girl presented to the emergency of the gynecology department of Lady Hardinge Medical College with a complaint of acute pain abdomen for 1 day. She had dull aching pain and a swelling in the lower abdomen for the last 10–12 days associated with decreased appetite and weight loss. There was no complaint of vomiting. She attained menarche 12 days back with normal menstrual flow. There was no history of tuberculosis in the past or any other chronic illness.
On examination, patient looked cachectic, was dehydrated and pallor was present. Her vitals were pulse rate 120 bpm, blood pressure 90/60 mmHg, respiratory rate 28/min, SpO2 98%, and temperature 101.2°F. Abdominal examination revealed a distended tense abdomen with guarding, rigidity, and rebound tenderness all over the abdomen. A fixed mass corresponding to 24-week gravid uterus size with variegated consistency was palpable in the lower abdomen.
Pelvic ultrasound examination revealed a hypodense cystic lesion measuring 81 mm × 121 mm displacing uterus to the right side. There was also the presence of moderate free fluid with internal echoes suggestive of hemorrhage.
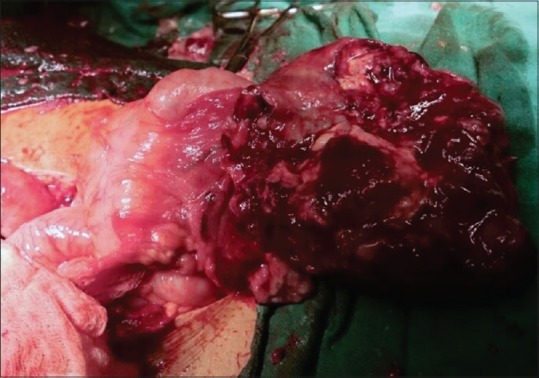
The patient was taken up for emergency exploratory laparotomy, and one liter of hemoperitoneum was drained. There was a large ruptured left ovarian mass of 10 cm × 12 cm with necrotic tissue coming out of it [Figure 1] with two twists around the pedicle. Another metastatic deposit of 6 cm × 6 cm was present on the omentum [Figure 2]. Uterus, right tube, and ovary were normal looking. Surgical stage 3C was assigned to the patient. A left salpingo-oophorectomy was done with total omentectomy, and the patient was given two units packed cells and four units fresh frozen plasma. The histopathological examination of the mass revealed yolk sac tumor stage T3NX. The tumor markers were done postoperatively and showed beta human chorionic gonadotropin 3.08 mIU/L, alpha-fetoprotein 337.55 ng/ml, lactate dehydrogenase 414 IU/L, and ca 125 42.07 U/ml. Her abdominal contrast-enhanced computed tomography report in the postoperative period was suggestive of multiple vertebral bone metastatic deposits and para-aortic lymph nodes. The patient continued to have fever till day 28 of surgery which was managed, and on day 29, bleomycin, etoposide, paclitaxel (BEP) regimen of chemotherapy was started. The patient started developing ascites which was tapped intermittently to relieve her pain during chemotherapy. She gradually developed subacute intestinal obstruction and massive lower limb lymphedema which lead to decrease venous return. Sepsis and disseminated carcinoma lead to multiple organ dysfunction, and she succumbed to her illness.

| Figure 1:Ruptured ovarian tumor mass
| Figure 2:Malignant omental mass
Discussion
Ovarian tumors usually present with chronic abdominal pain, an abdominal mass, or distension, but in some cases, it may rupture or undergo torsion and present as acute abdomen. Liu et al. did analysis of ovarian masses in 203 adolescents in China. The main complaint was abdominal pain or abdominal distension of several months duration, with or without increasing severity in 117 patients (57.7%). Approximately, 10% of patients had ovarian torsion, and no ruptures were there.[5] Malignant ovarian tumor presenting with acute pain abdomen is a very rare entity, and till date, very few cases have been reported in literature.
Saha et al. reported a case of a 14-year-old girl who presented with acute abdominal pain with distension of abdomen. On laparotomy, it was a suspected malignant ovarian tumor stage IC, and ipsilateral salpingo-oophorectomy was done, and on histopathological examination, it was a juvenile granulosa cell tumor. It was not followed up with chemotherapy, and up to the time of reporting, the patient was healthy with no recurrence.[6] Sunita Sudhir et al. reported a case of immature teratoma of the ovary in a 14-year-old girl who presented with acute pain abdomen. On laparotomy, it was a ruptured malignant germ cell ovarian tumor, and unilateral salpingo-oophorectomy was done. It was stage 1, grade 3. The patient was put on BEP regimen and responded well to chemotherapy.[7] In yet another case reported by Daher et al., rupture of mixed germ cell tumor was detected in a 12-year-old girl who presented with acute pain abdomen, vomiting, and distension. Emergency laparotomy was performed, and it revealed a ruptured ovarian tumor with omental invasion, and ipsilateral salpingo-oophorectomy was done with omentectomy. It was then followed by cisplatin-based chemotherapy, and the patient responded well.[8] In our case, the patient presented with acute pain abdomen and an abdominal mass and was similarly taken up for emergency laparotomy, but poor general condition and disseminated carcinoma resulted in the poor patient outcome.
Conclusion
The authors conclude that it is imperative to sensitize the population toward the early consultation in cases of young girls with an abdominal mass and pain abdomen. This is necessary to pick up ovarian tumors at initial stages so that prompt therapy can be instituted and the prognosis can be improved in these patients.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
The authors would like to acknowledge Dr. Chitra Raghunandan, Director Professor for the technical guidance and the general support and Dr. Shilpa Pimparkar, senior resident for the technical help required in the management of the patient.
References
- Lim FK, Chanrachakul B, Chong SM, Ratnam SS. Malignant ovarian germ cell tumours: Experience in the National University Hospital of Singapore. Ann Acad Med Singapore 1998;27:657-61.
- Berek SS, Hacker NF. Practical Gynecologic Oncology. 2nd ed. Baltimore: Williams and Wilkins; 1994. p. 377-402.
- Hudson CN. Recent advance in treatment of ovarian cancer. In: Stallworthy J, Bourne G, editors. Recent Advances in Obstetrics and Gynaecology. 13th ed. Edinburgh: Churchill Livingstone; 1979. p. 277-94.
- Stepanian M, Cohn DE. Gynecologic malignancies in adolescents. Adolesc Med Clin 2004;15:549-68.
- Liu H, Wang X, Lu D, Liu Z, Shi G. Ovarian masses in children and adolescents in China: Analysis of 203 cases. J Ovarian Res 2013;6:47.
- Saha E, Biswas SK, Saha D. Juvenile granulosa cell tumor- A rare presentation. Mediscope 2014;1:36-9.
- Sunita Sudhir P, Mishra S, Choudary V, Komal. Ruptured malignant germ cell ovarian tumor in a 14 year old girl: A case report. J Evol Med Dent Sci 2014;3:10423-7.
- Daher AK, Kareem MA, Al Biati RK. Rupture ovarian germ cell tumour. A case report. Med J Babylon 2010;7:589-95.
| Figure 1:Ruptured ovarian tumor mass
| Figure 2:Malignant omental mass
References
- Lim FK, Chanrachakul B, Chong SM, Ratnam SS. Malignant ovarian germ cell tumours: Experience in the National University Hospital of Singapore. Ann Acad Med Singapore 1998;27:657-61.
- Berek SS, Hacker NF. Practical Gynecologic Oncology. 2nd ed. Baltimore: Williams and Wilkins; 1994. p. 377-402.
- Hudson CN. Recent advance in treatment of ovarian cancer. In: Stallworthy J, Bourne G, editors. Recent Advances in Obstetrics and Gynaecology. 13th ed. Edinburgh: Churchill Livingstone; 1979. p. 277-94.
- Stepanian M, Cohn DE. Gynecologic malignancies in adolescents. Adolesc Med Clin 2004;15:549-68.
- Liu H, Wang X, Lu D, Liu Z, Shi G. Ovarian masses in children and adolescents in China: Analysis of 203 cases. J Ovarian Res 2013;6:47.
- Saha E, Biswas SK, Saha D. Juvenile granulosa cell tumor- A rare presentation. Mediscope 2014;1:36-9.
- Sunita Sudhir P, Mishra S, Choudary V, Komal. Ruptured malignant germ cell ovarian tumor in a 14 year old girl: A case report. J Evol Med Dent Sci 2014;3:10423-7.
- Daher AK, Kareem MA, Al Biati RK. Rupture ovarian germ cell tumour. A case report. Med J Babylon 2010;7:589-95.