 PDF
PDF  Views
Views  Share
Share


Stomach metastasis of breast carcinoma mimicking primary gastric neoplasm on fluorodeoxy glucose-positron emission tomography-computed tomography
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2013; 34(02): 128-129
DOI: DOI: 10.4103/0971-5851.116217
Abstract
We present fluorodeoxy glucose positron emission tomography-computed tomography (FDG-PET/CT) findings in a case of breast carcinoma. The PET/CT findings in this case were suspicious of second primary neoplasm in the stomach. However, on endoscopic biopsy, the lesion was found to be stomach metastasis of breast carcinoma with estrogen receptor positivity. Stomach is a rare site of breast carcinoma metastasis. Our case suggests that it is difficult to distinguish a stomach metastasis of breast cancer from a primary gastric cancer on the basis of clinical and imaging features. However, this differential diagnosis must be kept in mind and it is important to make such distinction because of its implications on patient management.
Keywords
Breast carcinoma - estrogen receptor positive - fluorodeoxy glucose positron emission tomography-computed tomography - stomach metastasis - second primary neoplasmPublication History
Article published online:
20 July 2021
© 2013. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Abstract
We present fluorodeoxy glucose positron emission tomography–computed tomography (FDG-PET/CT) findings in a case of breast carcinoma. The PET/CT findings in this case were suspicious of second primary neoplasm in the stomach. However, on endoscopic biopsy, the lesion was found to be stomach metastasis of breast carcinoma with estrogen receptor positivity. Stomach is a rare site of breast carcinoma metastasis. Our case suggests that it is difficult to distinguish a stomach metastasis of breast cancer from a primary gastric cancer on the basis of clinical and imaging features. However, this differential diagnosis must be kept in mind and it is important to make such distinction because of its implications on patient management.
CASE REPORT
We present fluorodeoxy glucose positron emission tomography–computed tomography (FDG-PET/CT) findings in a 53-year-old woman, a case of ductal breast carcinoma, post-modified radical mastectomy status. Six years after surgery, she was found to have skeletal metastases and PET/CT was performed to evaluate baseline pre-chemotherapy disease status. PET/CT, along with skeletal metastases, revealed a hypermetabolic stomach thickening [Figure 1], which was reported as a possible primary gastric neoplasm. The patient had no abdominal symptoms. Endoscopic biopsy of this lesion demonstrated presence of breast carcinoma metastasis with estrogen receptor positivity [Figure 2]. Stomach metastasis of breast carcinoma is very rare.[1,2,3] Our case suggests that it is difficult to distinguish a stomach metastasis of breast cancer from a primary gastric cancer on the basis of clinical and imaging features. However, this differential diagnosis must be kept in mind, and it is important to make such distinction because of its implications on patient management.
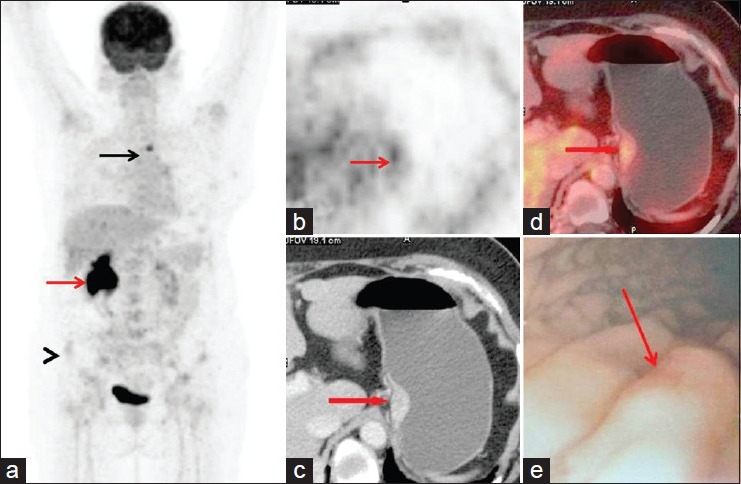
| Fig. 1 The PET/CT (a) showed increased FDG uptake in D3 vertebra (black arrow) and right iliac bone (black arrowhead), consistent with bone metastases. Non-specific tracer retention seen in right pelvicalyceal system is non-specific (red arrow). Focal FDG uptake (SUVmax = 4.6) was seen in stomach (b, arrow), which on CT and fused PET/CT localized to enhancing thickening along the lesser curvature of stomach extending 3 cm (c,d, arrows). These findings were suspicious of primary gastric neoplasm. Endoscopy revealed elevated lesion along lesser curvature of the stomach (e, arrow)
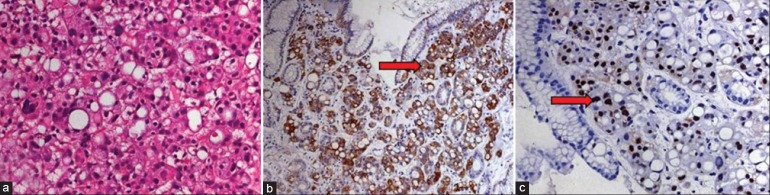
| Fig. 2 On histopathology, along with results of immunohistochemistry tests, the biopsied lesion was found to be metastasis of carcinoma breast, with strong expression of estrogen receptors. Photomicrograph of the pathology slides (a) shows ductal carcinoma of the breast. The neoplastic cells marked with arrows in b and c demonstrate positive staining for cytokeratin-7 (CK-7) and estrogen receptors (ER), respectively. Final diagnosis of stomach metastasis of breast carcinoma was made and the patient was started on hormonal therapy
Photomicrograph of the pathology slides (A) shows ductal carcinoma of the breast. The neoplastic cells marked with arrows in B and C demonstrate positive staining for cytokeratin-7 (CK-7) and estrogen receptors (ER), respectively. Final diagnosis of stomach metastasis of breast carcinoma was made and the patient was started on hormonal therapy.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
| Fig. 1 The PET/CT (a) showed increased FDG uptake in D3 vertebra (black arrow) and right iliac bone (black arrowhead), consistent with bone metastases. Non-specific tracer retention seen in right pelvicalyceal system is non-specific (red arrow). Focal FDG uptake (SUVmax = 4.6) was seen in stomach (b, arrow), which on CT and fused PET/CT localized to enhancing thickening along the lesser curvature of stomach extending 3 cm (c,d, arrows). These findings were suspicious of primary gastric neoplasm. Endoscopy revealed elevated lesion along lesser curvature of the stomach (e, arrow)
| Fig. 2 On histopathology, along with results of immunohistochemistry tests, the biopsied lesion was found to be metastasis of carcinoma breast, with strong expression of estrogen receptors. Photomicrograph of the pathology slides (a) shows ductal carcinoma of the breast. The neoplastic cells marked with arrows in b and c demonstrate positive staining for cytokeratin-7 (CK-7) and estrogen receptors (ER), respectively. Final diagnosis of stomach metastasis of breast carcinoma was made and the patient was started on hormonal therapy