 PDF
PDF  Views
Views  Share
Share


Synchronous Malignant Phyllodes Tumor with Skin Ulceration and Invasive Carcinoma as Collision Tumor
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2017; 38(01): 78-80
DOI: DOI: 10.4103/0971-5851.203499
Abstract
Phyllodes tumor is a rare fibroepithelial biphasic tumor of the breast composed of hypercellular mesenchymal stroma and double-layered epithelial component, arranged in clefts with leaf-like projections. Phyllodes tumor with coincidental presence of invasive carcinoma or in situ ductal carcinoma in the same or distinct breast is a rare occurrence, documented by some reports. Invasive carcinoma can be seen within or outside the phyllodes tumor. Skin ulceration by malignant phyllodes tumor with coexisting invasive carcinoma as collision tumor is extremely rare. Here, we report an extremely rare presentation of malignant phyllodes tumor as a giant fungating mass with distinct invasive carcinoma in the same breast in a 51-year-old female.
Keywords
Breast - fungating mass - invasive carcinoma - phyllodes tumor - skin ulceration - synchronousPublication History
Article published online:
06 July 2021
© 2017. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Abstract
Phyllodes tumor is a rare fibroepithelial biphasic tumor of the breast composed of hypercellular mesenchymal stroma and double-layered epithelial component, arranged in clefts with leaf-like projections. Phyllodes tumor with coincidental presence of invasive carcinoma or in situ ductal carcinoma in the same or distinct breast is a rare occurrence, documented by some reports. Invasive carcinoma can be seen within or outside the phyllodes tumor. Skin ulceration by malignant phyllodes tumor with coexisting invasive carcinoma as collision tumor is extremely rare. Here, we report an extremely rare presentation of malignant phyllodes tumor as a giant fungating mass with distinct invasive carcinoma in the same breast in a 51-year-old female.
Introduction
Phyllodes tumor of the breast accounts for 0.3%–1% of all primary breast tumors and for 2.5% of all fibroepithelial tumors of the breast.[1] They are circumscribed biphasic fibroepithelial tumors, with classic histology showing hypercellular mesenchymal stroma and double-layered epithelium in clefts. Periductal accentuation of stromal cells is characteristic. Based on stromal cellularity, atypia, mitosis and nature of tumor margins, phyllodes tumor is classified into benign, borderline, and malignant.[1,2] Most phyllodes tumor are benign with local recurrences in a small proportion of cases. Skin ulceration by phyllodes tumor is very rare.[1] Coexistence of invasive carcinoma in the proximity of malignant phyllodes tumor as synchronous collision tumors and skin ulceration by malignant phyllodes tumor is extremely rare. We report one such case in a 51-year-old female presenting as a fungating mass.
Case Report
A 51-year-old female presented with a history of breast lump for past 6 months. There was a history of rapid increase in size with pain and ulceration for 1 month. She had lost 6 kg of weight in 2 months. There was no history of breast malignancy in the family. On examination, left breast showed a huge foul smelling fungating mass with absent nipple and areola, occupying almost entire left breast. Axillary lymph nodes were palpable. Trucut biopsy elsewhere reported as phyllodes tumor. Mammogram was not done as the tumor was ulcerated. Positron emission tomography scan revealed large hypermetabolic mass in the left breast and few hypermetabolic lymph nodes in the left axilla. There was no evidence of metastasis elsewhere in the body. With the diagnosis of phyllodes tumor probably malignant with skin ulceration, mastectomy with axillary dissection was done.
Specimen revealed a large tumor ulcerating and erupting out through the skin. Nipple and areola were absent. The tumor measured 15.5 cm × 13 cm × 7 cm with lobulated margins. An another firm tumor measuring 2.5 cm with spiculated margin was seen at the periphery of large tumor, abutting it [Figure 1]. Histology of the larger tumor showed stromal predominance occupying a low power field [Figure 2], increased cellularity, spindle cells with moderate atypia, and increased mitosis [Figure 3] of 13/10 high power field (HPF). Scattered ducts in clefts and leaf like pattern were seen with double layered epithelium. Tumor was ulcerating the skin with surface necrosis. At its periphery, an epithelial tumor is seen without transition zone in between [Figure 4], consists of cells in tubules and trabeculae with stromal desmoplasiar [Figure 5]. Moderate atypia increased mitosis, and lymphovascular emboli were noted. Eleven axillary lymph nodes were involved by invasive carcinoma. A diagnosis of malignant phyllodes tumor with ulceration with coexisting invasive carcinoma of no special type was rendered. She was currently on chemotherapy and radiotherapy.

| Figure 1Gross specimen showing large lobulated phyllodes tumor (gray arrow) and a spiculated tumor at its proximity (black arrow)
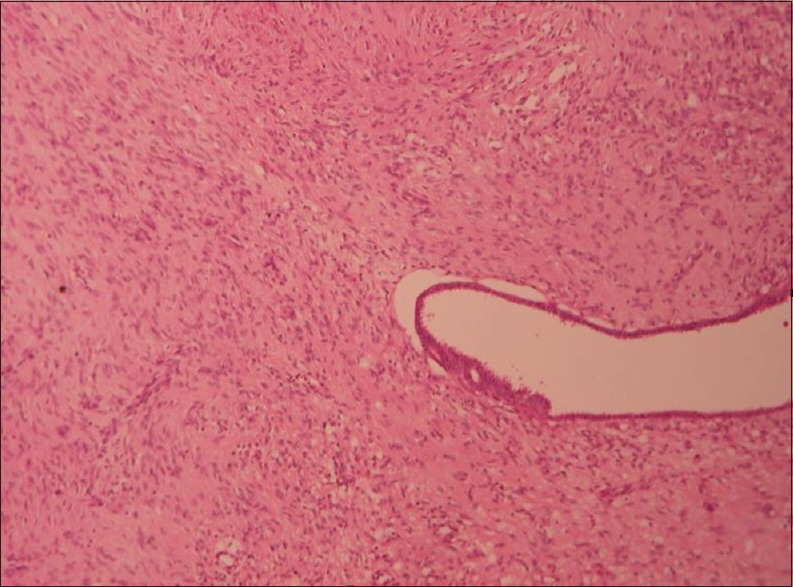
| Figure 2Low-power view of phyllodes tumor showing stromal predominance and epithelial cleft (H and E, ×10)
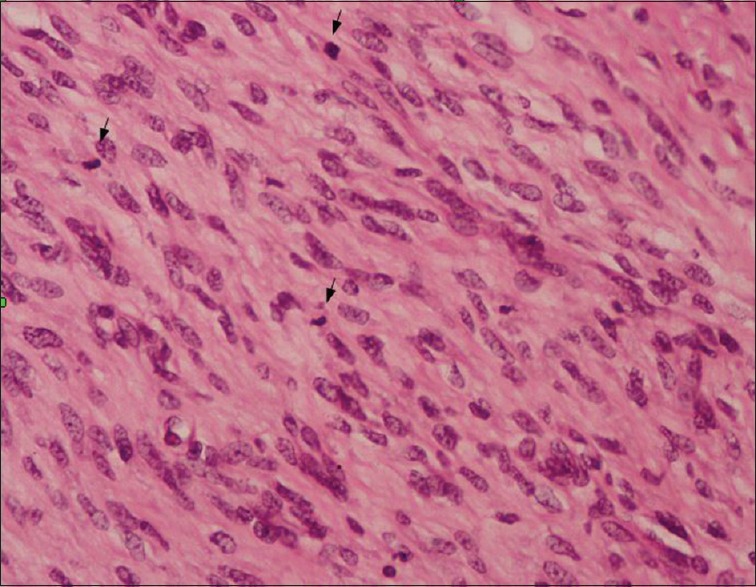
| Figure 3Phyllodes tumor showing hypercellular stroma and increased mitosis (arrows) (H and E, ×40)
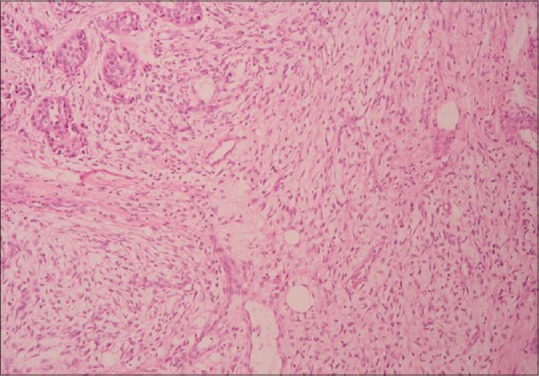
| Figure 4Phyllodes tumor merging with invasive carcinoma of no special type (H and E, ×10)
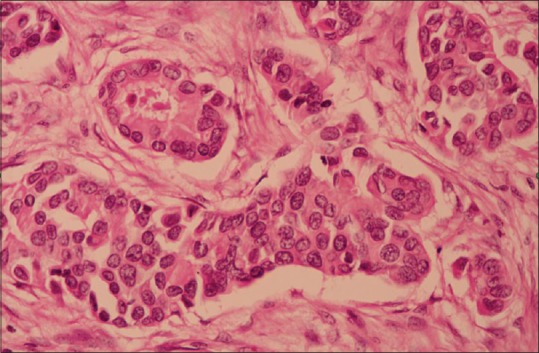
| Figure 5Invasive carcinoma showing tumor cells in nests and tubules (H and E, ×40)
Discussion
Phyllodes tumor is a biphasic fibroepithelial tumor of the breast, accounting for 0.3%–1% of all primary breast tumors and for 2.5% of all fibroepithelial tumors of the breast. It occurs in women, predominantly in the fourth to fifth decade of life. They develop de novo, from intralobular or periductal stroma.[1,2] Clinically, patients present with unilateral firm breast mass, not attached to skin. Large tumors might stretch the skin,[1] but ulceration is very rare (seen in our case). Imaging reveals a rounded, usually sharply defined hypoechoic mass with macrolobulations.[3]
Phyllodes tumor is classified based on stromal cellularity, stromal atypia, stromal overgrowth, mitosis and tumor margins into benign, borderline, and malignant.[1,2] Malignant phyllodes tumor can show heterologous sarcomatous component. Any phyllodes tumor can harbor ductal carcinoma in situ or invasive carcinoma, although it is an uncommon finding.[4] The epithelial tumor can be seen either with or outside the phyllodes tumor, synchronously, or metachronously, in the same or distinct breast.[5,6] Very rare cases of malignant phyllodes tumor with coexisting invasive carcinoma outside the phyllodes tumor in the same breast were described.[6,7] Our patient had invasive carcinoma in the proximity of phyllodes tumor without a transition zone synchronously in the same breast as a collision tumor.
The pathogenesis behind the association of phyllodes tumor and breast carcinoma is unknown. Genetic changes with intratumoral heterogeneity have been reported, which might lead to the transformation of epithelial and mesenchymal elements, resulting in the development of phyllodes tumor and the association of breast carcinoma inside the phyllodes tumor.[7,8] This cannot explain the pathogenesis of breast carcinoma outside phyllodes tumor. The association could be coincidental.[7]
The coexistence of both tumors can be made out by meticulous examination of the specimen and extensive sampling. The appearance of tumor and consistency varies. Phyllodes tumor have homogenous surface with lobulated margins, while breast carcinoma usually has firm consistency with spiculated margins.
Histologically, malignant phyllodes tumor reveal stromal overgrowth occupying more than a low-power field, hypercellularity, stromal atypia, mitosis of more than 10/10 HPF, and invasive margins. It can have malignant heterologous elements even in the absence of other features. Local recurrence is usual and can metastasize to lungs, liver, and bone by hematogenous spread.[1,2]
Invasive breast carcinoma is a tumor originating from the terminal ductal-lobular unit. It is graded based on the amount of tubule formation, nuclear atypia, and mitosis per 10 HPF.[1,2] It usually metastasize to axillary lymph nodes, and to other organs such as lungs and bone. The behavior of the tumor and treatment depends on the higher grade of either of the tumors, mitotic activity, resected margin status, skin involvement, and metastasis.[1,2]
Conclusion
Malignant phyllodes tumor with coexisting invasive breast carcinoma in the same breast outside the phyllodes tumor is a rare occurrence. There were two case reports of malignant phyllodes tumor ulcerating the skin with coexisting invasive breast carcinoma as collision tumor and presenting as a large fungating mass in the English literature.[6,7] Early diagnosis and complete surgical removal prevent the recurrence of such tumors and improve patient outcome. Treatment of these rare cases has to be standardized with a multimodal approach, including complete surgical removal with axillary clearance, and adjuvant treatment with chemotherapy and radiotherapy as well.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Lakhani SR, Ellis IO, Schnitt SJ, Tan PH, van de Vijver MJ, editors. WHO Classification of Tumours of the Breast. 4th ed.. Lyon: IARC; 2012. p. 143-7.
- Rosen PP, editors. Fibroepithelial neoplasms. In: Rosen's Breast Pathology. 3rd ed.. Philadelphia: Lippincott Williams and Wilkins; 2009. p. 187-229.
- Tan H, Zhang S, Liu H, Peng W, Li R, Gu Y, et al. Imaging findings in phyllodes tumors of the breast. Eur J Radiol 2012;81:e62-9.
- Panda KM, Naik R. A Clinicopathological study of benign phyllodes tumour of breast with emphasis on unusual features. J Clin Diagn Res 2016;10:EC14-7.
- Sato T, Muto I, Sakai T. Coexistence of malignant phyllodes tumor and her2-positive locally advanced breast cancer in distinct breasts: A case report. Int J Surg Case Rep 2016;19:163-7.
- Shin YD, Lee SK, Kim KS, Park MJ, Kim JH, Yim HS, et al. Collision tumor with inflammatory breast carcinoma and malignant phyllodes tumor: A case report and literature review. World J Surg Oncol 2014;12:5.
- Macher-Goeppinger S, Marme F, Goeppert B, Penzel R, Schirmacher P, Sinn HP, et al. Invasive ductal breast cancer within a malignant phyllodes tumor: Case report and assessment of clonality. Hum Pathol 2010;41:293-6.
- Sawyer EJ, Hanby AM, Ellis P, Lakhani SR, Ellis IO, Boyle S, et al. Molecular analysis of phyllodes tumors reveals distinct changes in the epithelial and stromal components. Am J Pathol 2000;156:1093-8.
| Figure 1Gross specimen showing large lobulated phyllodes tumor (gray arrow) and a spiculated tumor at its proximity (black arrow)
| Figure 2Low-power view of phyllodes tumor showing stromal predominance and epithelial cleft (H and E, ×10)
| Figure 3Phyllodes tumor showing hypercellular stroma and increased mitosis (arrows) (H and E, ×40)
| Figure 4Phyllodes tumor merging with invasive carcinoma of no special type (H and E, ×10)
| Figure 5Invasive carcinoma showing tumor cells in nests and tubules (H and E, ×40)
References
- Lakhani SR, Ellis IO, Schnitt SJ, Tan PH, van de Vijver MJ, editors. WHO Classification of Tumours of the Breast. 4th ed.. Lyon: IARC; 2012. p. 143-7.
- Rosen PP, editors. Fibroepithelial neoplasms. In: Rosen's Breast Pathology. 3rd ed.. Philadelphia: Lippincott Williams and Wilkins; 2009. p. 187-229.
- Tan H, Zhang S, Liu H, Peng W, Li R, Gu Y, et al. Imaging findings in phyllodes tumors of the breast. Eur J Radiol 2012;81:e62-9.
- Panda KM, Naik R. A Clinicopathological study of benign phyllodes tumour of breast with emphasis on unusual features. J Clin Diagn Res 2016;10:EC14-7.
- Sato T, Muto I, Sakai T. Coexistence of malignant phyllodes tumor and her2-positive locally advanced breast cancer in distinct breasts: A case report. Int J Surg Case Rep 2016;19:163-7.
- Shin YD, Lee SK, Kim KS, Park MJ, Kim JH, Yim HS, et al. Collision tumor with inflammatory breast carcinoma and malignant phyllodes tumor: A case report and literature review. World J Surg Oncol 2014;12:5.
- Macher-Goeppinger S, Marme F, Goeppert B, Penzel R, Schirmacher P, Sinn HP, et al. Invasive ductal breast cancer within a malignant phyllodes tumor: Case report and assessment of clonality. Hum Pathol 2010;41:293-6.
- Sawyer EJ, Hanby AM, Ellis P, Lakhani SR, Ellis IO, Boyle S, et al. Molecular analysis of phyllodes tumors reveals distinct changes in the epithelial and stromal components. Am J Pathol 2000;156:1093-8.