 PDF
PDF  Views
Views  Share
Share


Unusual Presentation of Metanephric Stromal Tumor in a Neonate
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2017; 38(03): 357-359
DOI: DOI: 10.4103/ijmpo.ijmpo_27_16
Abstract
Metanephric stromal tumor (MST) of kidney is an under-reported benign stromal specific renal neoplasm with good prognosis. This tumor is to be differentiated from congenital mesoblastic nephroma and clear-cell sarcoma of the kidney. In this case report, we describe the imaging, gross, and microscopic features of MST with ischemic left kidney in a 1-month-old child and discuss treatment with relevant literature.
Keywords
Atypical Wilms tumor - congenital mesoblastic nephroma - metanephric stromal tumor - pediatric renal tumorPublication History
Article published online:
04 July 2021
© 2017. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Abstract
Metanephric stromal tumor (MST) of kidney is an under-reported benign stromal specific renal neoplasm with good prognosis. This tumor is to be differentiated from congenital mesoblastic nephroma and clear-cell sarcoma of the kidney. In this case report, we describe the imaging, gross, and microscopic features of MST with ischemic left kidney in a 1-month-old child and discuss treatment with relevant literature.
Introduction
Stromal tumors of the kidney form 15% of the pediatric renal tumors. Metanephric stromal tumo (MST), a purely stromal specific renal neoplasm, has a characteristic microscopic appearance that helps differentiate between congenital mesoblastic nephroma (CMN) and clear-cell sarcoma of kidney (CCSK). Complete excision is curative in most cases of MST. The differentiation of MST from CCSK is very important as it will spare the child from the adjuvant chemotherapy.
Case Report
A 30-day-old neonate delivered vaginally and discharged home was brought again to hospital 8 days after discharge with lethargy, poor feeding. The baby was admitted and found to have hypoglycemia and hypertension on admission. Blood tests revealed raised serum creatinine (1.07), hemoglobin 11.3, total count 13,200, and normal platelet count. The baby was started on antihypertensive medications. After stabilizing general condition, renal ultrasound was done which revealed 1.7 cm × 1.2 cm heterogeneously hypoechoic lesion at the left renal hilum superior to hilar vessels with no vascularity, ? neoplastic etiology. Doppler examination showed left kidney appearing ischemic with minimal flow within collaterals.
Urine vanillylmandelic acid levels were normal; plasma metanephrine levels were mildly raised. Fundoscopy was normal. Computed tomography (CT) showed left kidney 4.3 cm × 2.6 cm in size with no nephrogram and no contrast excretion seen. An ill-defined isodense lesion 1.1 cm × 0.9 cm seen in left renal hilum with few calcific specks [Figures [Figures11 and and22].

| Figure 1:Peripheral smear showing presence of blast cells

| Figure 2:Computed tomography showed no nephrogram and no contrast excretion on the left side
Patient's blood pressure was controlled with antihypertensive medications and posted for excision of left renal hilar mass and if needed proceeding with left nephrectomy. Intraoperatively, an ischemic left kidney with hilar mass was found. Left nephrectomy was done with excision of hilar mass [Figures [Figures33 and and44].
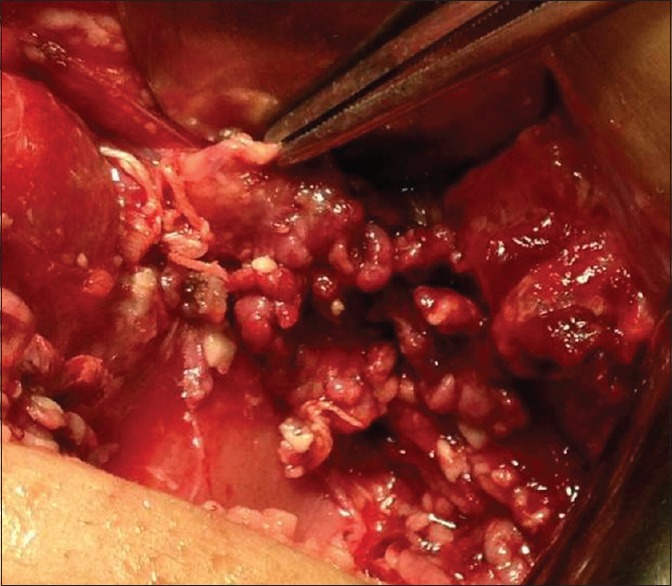
| Figure 3:Intraoperative photo showing hilar mass

| Figure 4:Specimen of left nephrectomy with hilar mass
The patient had an uneventful recovery and gradually tapered off from antihypertensive medications.
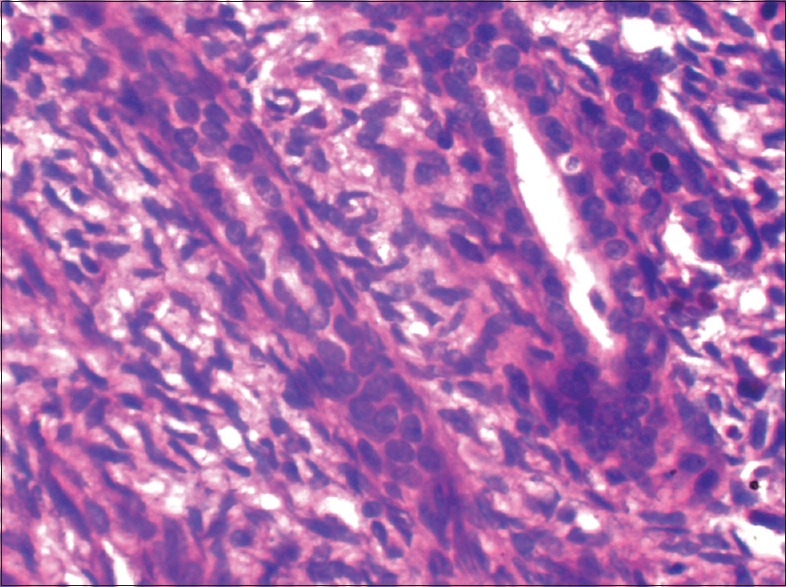
Histopathological examination showed spindle cells in fascicles, cells having elongated nuclei with infiltrating borders. Mitotic figures were not seen [Figure 5]. The spindle cells were wrapped around immature renal tubules in an onion skin fashion. Blood vessels entrapped among the stromal cells showed medial hypertrophy. Stromal cells arranged around the tubules showed positivity for CD34, demonstrating the immature nature of these cells. Left hilar mass contained blood vessels with thrombus with surrounding connective tissue nerve bundles [Figure 6].
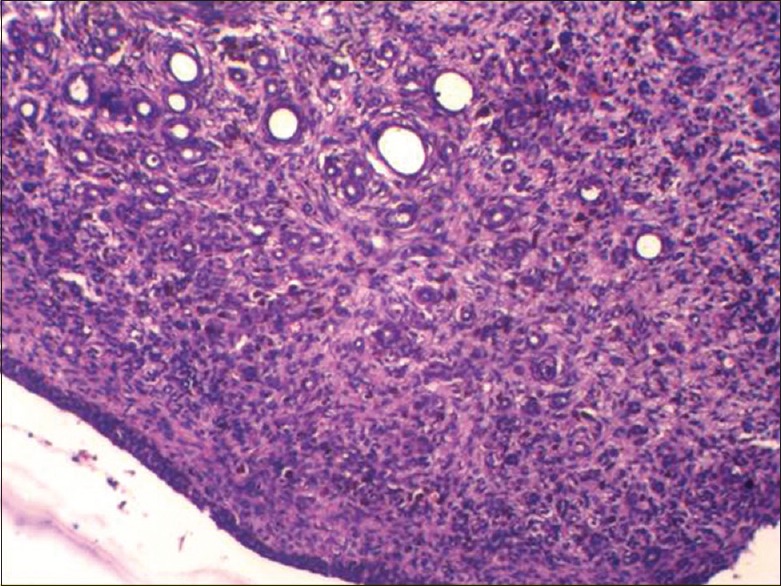
| Figure 5:Histopathological examination showing spindle cells in fascicles, cells having elongated nuclei with infiltrating borders
| Figure 6:Left hilar mass found to contain blood vessels with thrombus with surrounding connective tissue nerve bundles
The patient was discharged without the need for chemotherapy.
Discussion
Congenital renal tumors comprise 2.5%–7% of all perinatal tumors. These include in decreasing order of frequency, CMN, Wilms tumor, rhabdoid tumor, clear cell sarcoma of kidney, hamartomas, and ossifying tumor of infancy. MST is an under-reported pediatric pure stromal neoplasm of kidney with good prognosis. MST occurs in early infancy and childhood (median age 13 months and peak at 2 years). Isolated cases have been reported in adults also. MST along with metanephric adenofibroma and metanephric adenoma represents a spectrum of well-differentiated nephroblastic lesions that appear to be related to Wilms tumor.[1] Argani and Beckwith[2] reported 31 cases of MST in their series with a benign course. Complete excision alone is curative in most cases. MST should be differentiated from CCSK as it will spare the child from the enfeebling side effects of adjuvant chemotherapy. MST is usually centered in the renal medulla, but one case of its continuous extension through the bladder to the prostatic urethra was found.[3] Microscopically, this neoplasm is an unencapsulated lesion that entraps native kidney. Under low power, it has a nodular appearance. Onion skin cuffing (collarettes) and angiodysplasia of intratumoral vessels are the distinctive features of MST. MSTs present as abdominal mass or incidental finding. Hypertension as a complication of MST in the neonate has not been reported in literature. The outlook following surgical nephrectomy is excellent with no reported recurrence/metastasis compared to atypical Wilms and CCSK which metastasize widely while even RRT and cellular CMN occasionally metastasize. The confirmation of the diagnosis is based only on histopathological features and immunohistochemistry (CD34 and vimentin). It is difficult to diagnose MST on imaging characteristics alone. MST should be suspected in a young child having unencapsulated unilateral renal tumor with central cystic component and presence of heterologous tissues like cartilage, glial tissue, bone on computed tomography. Postnephrectomy, the specimen must be examined for CD34 positivity which will help distinguish it from CCSK.
Conclusion
MST is a rare tumor; many clinicians, radiologists, and pathologists may not come across even a single case in their lifetime, but their importance lies in their extremely benign nature and good prognosis after nephrectomy without need for chemotherapy.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Argani P, Beckwith JB. Renal neoplasms of childhood. In: Mills SE, editor. Sternbergs Diagnostic Surgical Pathology. 4th ed. Philadelphia: Lippincot Williams and Wilkins; 2004. p. 2029-30.
- Argani P, Beckwith JB. Metanephric stromal tumor: Report of 31 cases of a distinctive pediatric renal neoplasm. Am J Surg Pathol 2000;24:917-26.
- Lorenzo AJ, Timmons C, Weinberg A, Megison SM, Snodgrass WT. Metanephric stromal tumor with urothelial extension. J Urol 2003;169:1095-7.
| Figure 1:Peripheral smear showing presence of blast cells
| Figure 2:Computed tomography showed no nephrogram and no contrast excretion on the left side
| Figure 3:Intraoperative photo showing hilar mass
| Figure 4:Specimen of left nephrectomy with hilar mass
| Figure 5:Histopathological examination showing spindle cells in fascicles, cells having elongated nuclei with infiltrating borders
| Figure 6:Left hilar mass found to contain blood vessels with thrombus with surrounding connective tissue nerve bundles
References
- Argani P, Beckwith JB. Renal neoplasms of childhood. In: Mills SE, editor. Sternbergs Diagnostic Surgical Pathology. 4th ed. Philadelphia: Lippincot Williams and Wilkins; 2004. p. 2029-30.
- Argani P, Beckwith JB. Metanephric stromal tumor: Report of 31 cases of a distinctive pediatric renal neoplasm. Am J Surg Pathol 2000;24:917-26.
- Lorenzo AJ, Timmons C, Weinberg A, Megison SM, Snodgrass WT. Metanephric stromal tumor with urothelial extension. J Urol 2003;169:1095-7.