 PDF
PDF  Views
Views  Share
Share


Tobacco-related cancers in India: A review of incidence reported from population-based cancer registries
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2016; 37(03): 152-157
DOI: DOI: 10.4103/0971-5851.190357
Abstract
Background: Tobacco related cancers (TRC) account for major share of all cancers and updated of incidence data are helpful in policy changes. The aim was to present an update of TRCs on age-adjusted incidence data and corresponding lifetime risk of developing TRC for different regions of the country. Methods: The data for this study were obtained from published reports of 25 population-based cancer registries (PBCRs) in India. The PBCRs in different parts of India were divided into seven regions such as North, South, Central, Northeast, West, Rural West, and East. Data indicators such as age-adjusted rates (AARs) of incidence and the cumulative risks of TRCs up to the age of 64 years for each of the 10 TRC sites of either sex in each of 25 registries were obtained from the National Cancer Registry Programme reports. Results: Among all TRCs, esophagus, lung, hypopharynx, and mouth are the leading sites for both males and females. Males in Northeast region had the highest risk 1 in 27 of developing esophageal cancer, 1 in 67 for cancer of lungs and hypopharynx, followed by 1 in 143 for both mouth and tongue cancers. Females also had the highest risk of esophagus and lungs (1 in 63 female) and cancer of mouth (1 in 250) in Northeast region. Proportion of TRC in comparison of all cancer ranged from 11–25% for men and 3–18% for women. Conclusions: Proportion of TRC in relation to all cancers was still high in different registries of India including the Northeast region.
Keywords
Cancer registry - incidence - India - population-based cancer registries - tobacco-related cancersPublication History
Article published online:
12 July 2021
© 2016. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Abstract
Background:
Tobacco related cancers (TRC) account for major share of all cancers and updated of incidence data are helpful in policy changes. The aim was to present an update of TRCs on age-adjusted incidence data and corresponding lifetime risk of developing TRC for different regions of the country.
Methods:
The data for this study were obtained from published reports of 25 population-based cancer registries (PBCRs) in India. The PBCRs in different parts of India were divided into seven regions such as North, South, Central, Northeast, West, Rural West, and East. Data indicators such as age-adjusted rates (AARs) of incidence and the cumulative risks of TRCs up to the age of 64 years for each of the 10 TRC sites of either sex in each of 25 registries were obtained from the National Cancer Registry Programme reports.
Results:
Among all TRCs, esophagus, lung, hypopharynx, and mouth are the leading sites for both males and females. Males in Northeast region had the highest risk 1 in 27 of developing esophageal cancer, 1 in 67 for cancer of lungs and hypopharynx, followed by 1 in 143 for both mouth and tongue cancers. Females also had the highest risk of esophagus and lungs (1 in 63 female) and cancer of mouth (1 in 250) in Northeast region. Proportion of TRC in comparison of all cancer ranged from 11–25% for men and 3–18% for women.
Conclusions:
Proportion of TRC in relation to all cancers was still high in different registries of India including the Northeast region.
INTRODUCTION
Cancer is a leading cause of disease worldwide with an estimated 14.1 million new cancer cases occurring in 2012.[1] Seventeen million new cases are expected worldwide by 2020 with three-fourth of the cancer-related deaths occurring in developing countries of the world.[2] Out of all cancers, tobacco-related cancer (TRC) accounts for major share. If the current trends in smoking and population growth continue, the number of current smokers is expected to reach 2 billion worldwide by 2030.[3] With the decline of tobacco use in many industrialized countries, the geography of smoking has shifted from the developed to the developing world, especially for men. About 50% of men and 9% of women are current smokers in developing countries, compared with 35% of men and 22% of women in high-resource countries.[4]
The WHO estimates that one out of two young people who start smoking and continue smoking throughout their lives will lead to TRC.[3] Hence, TRC's deserve a closure monitoring of incidence to prioritize the medical care resources and plan the cancer control programs. A study on the risk of developing cancer in India in the age group of 35–70 + years showed that the probability of developing tobacco related cancers was high in males (4.75%) as compared to females (2.16%). The study also stated that out of the total cancer cases nearly 45% in males and 20% in females are due to tobacco use.[5]
The proportion of TRCs in India in relation to other cancers ranges from 35% (Bengaluru) to 50% (Bhopal) among males. Trend for TRCs in various major cancer registries are reported from North east cancer registry of India.[6,7] Cancer related to tobacco use is preventable through primary prevention. Reporting burden of TRCs from time to time in respect to geographical distribution of Indian population-based cancer registries (PBCRs) data would be helpful for action on preventive measures through policies related to control of disease. The study presents an update of incidence data of TRCs from a recent report of National Cancer Registry Programme (NCRP) in the form of age-adjusted incidence rate (AAR) and an easily understandable parameter on magnitude of lifetime risk of developing TRC for different regions of the country.
METHODS
The data for this study obtained from published reports of 25 PBCRs in India.[8] The reports are compiled by NCRP of Indian Council of Medical Research (ICMR), and data are available in public domain. Cancer registries cover different parts of India for urban and rural populations. The PBCRs in different parts across the country were divided into seven regions for the purpose of the present study as reported earlier by us.[9,10] The regions were as follows – North: Delhi; South: Bengaluru, Chennai, Kollam, Thiruvananthapuram; Central: Bhopal; Northeast: Cachar District, Kamrup urban District, Manipur State, Mizoram, Nagaland, Meghalaya, Sikkim, and Tripura State; West: Mumbai, Nagpur, Pune, Ahmedabad (urban), and Barshi; (extended); Rural West: Barshi (rural) and Ahmedabad (rural); and East: Kolkata.
Data on all the important sites of cancer considered to be tobacco related were selected. The data on ten TRC sites (along with International Classification of Diseases code) collected from each cancer registry were lip (C00), tongue (C01–C02), mouth (C03–C06), oropharynx (C10), hypopharynx (C12–C13), pharynx (C14), esophagus (C15), larynx (C32), lung (C33–C34), and urinary bladder (C67).
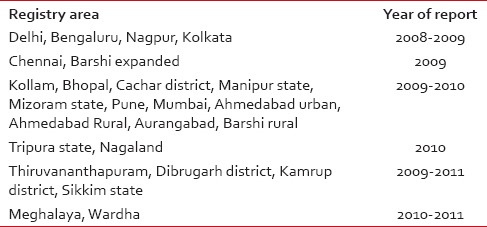
Data indicators such as age-adjusted rates (AARs) of incidence and the cumulative risks of TRCs up to age of 64 years for each of the ten TRC sites of either sex in each of 25 registries were obtained from NCRP source. The indicators computed by NCRP were based on the following formulae: *Cumulative risk = 100× (1 − exp [−cumulative rate/100]). Where cumulative rate = (5× Σ [ASpR] ×100)/100000 and ASpR is age-specific incidence rates. An easy to understand epidemiological indicator, one in a number of persons likely to develop TRC in the lifetime during 0–64 years was computed by us for each TRC site in each registry. The indicator for one in a number of persons likely to develop TRC site was calculated by 100/cumulative risk. Data on indicators, namely AARs and one in number of persons develop cancer were summarized for both the sexes in each of the cancer registries were presented region-wise in the form of ranges. Year of data reporting for various registries was as given in Table 1.[8]
Table 1
Registry area for data collected on tobacco-related cancer from population-based cancer registry reports according to year of report[8]
RESULTS
The indicators of AARs and one in a number of persons likely to develop cancer for all TRC sites in 0–64 years of age were presented for men and women, respectively, in Tables Tables22 and and3.3. For all regions, the incidence of TRC for men and women was highest in Northeast region of India. For men, it was 46/100,000, and for women, it was 29/100,000. The next highest magnitude was observed in Southern and Western regions. The lowest incidence of TRC for men and women was found to be in rural West region. The overall risk of TRC as one in number of persons likely to develop tobacoo related cancer ranged from 1 in 27 to 1 in 143 for men and 1 in 63 to 1 in 333 for women.
Table 2
Incidence of tobacco-related cancers in different geographical regions of India categorized according to location of population-based cancer registry in females
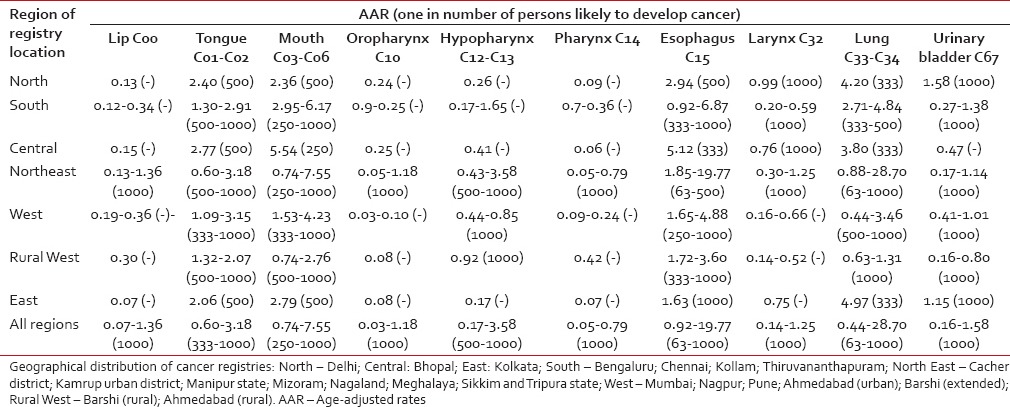
Table 3
Incidence of tobacco-related cancers in different geographical regions of India categorized according to location of population-based cancer registries in males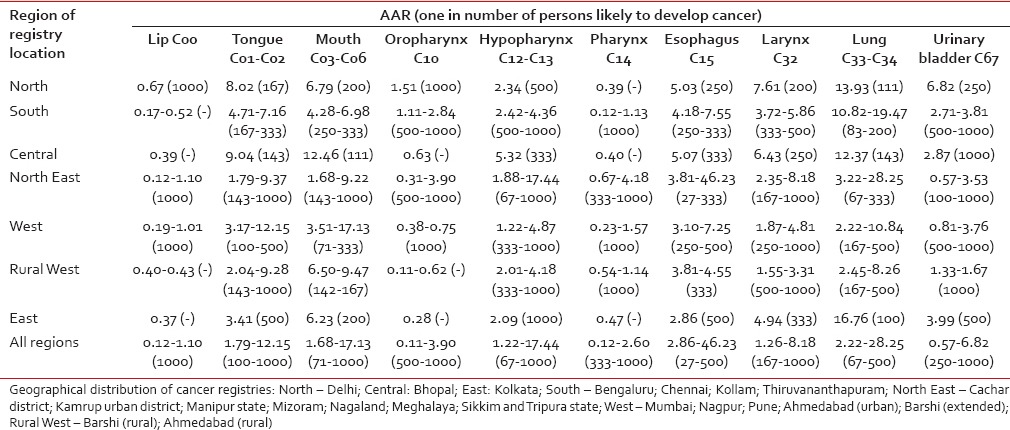 Development of esophageal cancer was of maximum risk with 1 in 27, followed by 1 in 67 for cancer of the lungs and hypopharynx observed in the Northeastern regions [Table 2]. This was followed by 1 in 83 being at risk to develop lung cancer in men of Southern region and 1 in 63 being at risk to develop lung cancer in the Northeastern region. The incidence of lip cancer was the least in all the regions of the country with 1 in 1000. The risk was 1 in 143 for both mouth and tongue cancers in Northeast region. In the Southern region, risk for TRC was 1 in 83 for developing lung cancer and 1 in 167 for tongue cancer. Risk in Western region was 1 in 71 for mouth cancer followed by, 1 in 100 for cancer of tongue and 1 in 167 for cancer of lung.
Development of esophageal cancer was of maximum risk with 1 in 27, followed by 1 in 67 for cancer of the lungs and hypopharynx observed in the Northeastern regions [Table 2]. This was followed by 1 in 83 being at risk to develop lung cancer in men of Southern region and 1 in 63 being at risk to develop lung cancer in the Northeastern region. The incidence of lip cancer was the least in all the regions of the country with 1 in 1000. The risk was 1 in 143 for both mouth and tongue cancers in Northeast region. In the Southern region, risk for TRC was 1 in 83 for developing lung cancer and 1 in 167 for tongue cancer. Risk in Western region was 1 in 71 for mouth cancer followed by, 1 in 100 for cancer of tongue and 1 in 167 for cancer of lung.Northeast region was at the highest risk of developing TRC for women [Table 3]. The maximum risk was found in lung and esophageal carcinomas (1 in 63 being at risk) followed by mouth mouth (1 in 250 being at risk). In the Western region, the highest risk of developing TRC of various sites was 1 in 333 for tongue as well as mouth cancers. Both Southern and Central regions showed highest risk of developing TRC with risk of 1 in 250 for mouth cancer and 1 in 333 for cancer of hypopharynx in western region.
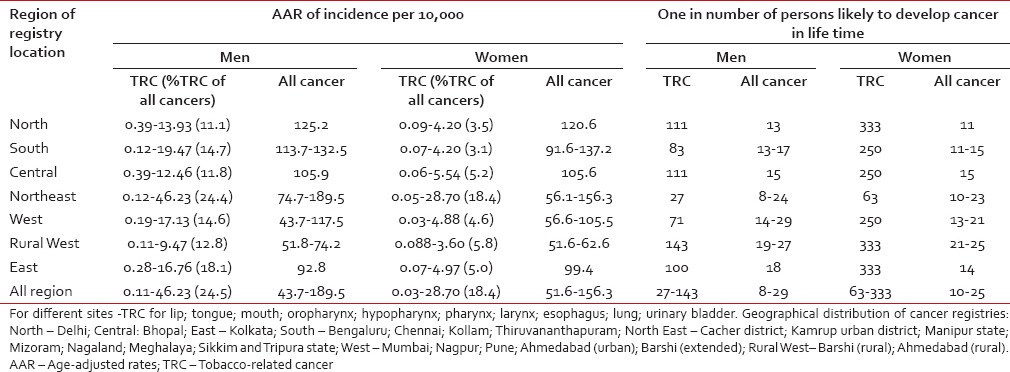
Incidence of TRCs versus all cancers among men and women in different regions of India according to the location of cancer registry is shown in Table 4. Proportion of TRC in comparison of all cancer ranged from 11–25% for men and 3–18% for women.Table 4
Incidence of tobacco-related cancers versus all cancers among men and women in different regions of India according to the location of cancer registry
DISCUSSION
The recent NCRP data on TRC analyzed in the present study revealed that up to one-fourth of all cancers among men and little lower than one-fifth among women were tobacco related. The maximum incidence among men was reported for esophagus, lungs, and hypopharynx cancers from the Northeast of India and mouth cancer for Western India. Among women, maximum rates were reported for esophagus and lung cancers in Northeast region. In comparison to earlier year data, there has been a reduction in the proportion of TRC to all cancers in both men and women based on the present data from 25 PBCRs of India. The share of TRC from all cancers observed to be reduced to 25% in the present study as compared to 61% reported for the year 2003–2004 for Northeast region.[7] Such reduction was also evident when compared with all other registries.[6] The overall risk of developing TRC was highest in the Northeast region compared to all other regions. A study compared between the overall incidence of all cancer cases from Northeast region and other regions from India observed higher cancer incidence in Northeast. The study also compared Northeast cancer incidence data with global data but found its similarities with the Southeast Asian region. The conclusion is that genetic pool of Northeast region of India is different from rest of the country but resembles with Southeast Asian region linkage.[11] Our earlier communication on review from the first North East Cancer Registry Report also reported a high incidence of cancer in Northeast region for both men and women.[7] Second highest magnitude TRC was for West region for both men and women. There are results from global studies using cancer registry data on geographical distributions of TRCs. A study from Cyprus reported TRCs in Cyprus and compared AARs in rural and urban districts and also compared the data with the data of many other European countries.[12] A study on upper gastrointestinal cancers clustering and geographical variation in North China found a difference in various geographical areas is due to regional differences.[13]
Among all important TRC sites, the risk of getting lung cancer was higher in most regins of the country and oesophageal cancer was highest for both men and women of North eastern region. A study from Kamrup urban cancer registry of Northeast India reported esophagus was the leading site of cancer among men with an age-adjusted rate of 30.7/100,000 among men.[14] In another study from Kamrup district reported that among upper aerodigestive tract cancer of esophagus as a most common site in both sexes.[15] Lung cancer was important site for women and this was a most commonly occurring cancer and its risk was equal to the risk of getting oesophageal cancer. Lung and hypopharynx cancers were the second most common site among men with risk of one out of every 67. The cancer registry data for 2001–2004 from India reported highest for lung cancer followed by esophagus and larynx.[16] Ranking in the site of cancer has been altered after incorporation of data of recent population-based cancer registry into the study. Mouth cancer was another leading cause in both men (one in 71) and women (one in 250). Although the risk of mouth cancer in women was less as compared to men, it was ranking the second highest TRC among women.
A study from registry data on temporal changes in relation to gender observed declining proportion of TRCs between the years 1990–96 and 2003 for all registries except Bhopal.[17] This earlier study considered data for 12 PBCRs, whereas present study reported data on 25 PBCRs from 2009 to 2011 reports. Our earlier report for the year 2000 using data on only six major PBCRs had shown increasing trends of esophageal cancer in males (Chennai city) and rising trends for lung cancer among females in Bengaluru, Chennai, and Mumbai since 1982.[6] The present study observed a reduction in percent of TRC out of all cancers as compared to data reported up to the year 2004 in various registries including Northeast registry where highest incidence was reported. This could be due to policies by Government of India for tobacco prevention and control and increase in general awareness among population related to health hazards of tobacco.[18] A study from Pakistan's Hyderabad showed that 40.0% of the tumors in males and 20.0% in females were TRCs.[19] A study from Gandhi Nagar district of Gujarat in India which collected raw data from various sources found that among males, 53% of cancers were tobacco related and emphasized the need for oral screening for early detection.[20] In a study from Kamrup district of Northeast percentage of TRCs for 2003–2008 is high for both males (58.2%) and females (26.9%).[14] In our study, we found percentage of TRC as high as 24.5% for men and 18.4% for women [Table 4]. The aforementioned lower percentage of TRCs in compare with other studies may be due to recent declining trend in TRCs. Reliability of data issues is important on the data collected across the registries. The limitation of the study is the time frame of data collection which is different in different areas due to nonavailability of data for uniform time frame [Table 1]. In different regions of the country, cancer registries’ are compiled under the network of ICMR through NCRP. All the registries under NCRP follow uniform data collection procedures. A study to assess the quality of data from Mumbai, India, stated some indicators that can throw some light on the quality of data collected by the registry.[21] For example, there has been a notable improvement in the percentages of histological verification of cases and a substantial decrease in the proportion of death certificate alone cases in both the sexes over a period of time. Mortality incidence ratio remained stable over a period of time in both the sexes. On examining the various indices of reliability and completeness of Mumbai cancer registry data, it is concluded that the data collected by this registry are quite complete and reliable.[21] In an NCRP report, mortality incidence ratio that is an important index of reliability for males and females ranged 11.8–82% and 7.1–73.1% for males and females, respectively.[8] The other measure is that of a good proportion of microscopically verified cases. This reported for the present study database was 61.5–93.9% and 56.4–94.4% for men and women, respectively. This shows a good proportion of microscopically verified cases as compared to the highest 89% in a previous report of NCRP.[22] In an independent survey in Chennai, Tamil Nadu, India, that assessed completeness of Chennai PBCR during 1982–1995 found 96% completeness as compared to that of the other registries in the world.[23] The data compiled by NCRP on the whole can be considered to be reliable.
The present study divided 25 PBCRs into different regions that were arbitrary in nature for the sake of ease in presentation. This kind of division may not cover the entire population of that region due to the diverse distribution in limited population coverage of those PBCRs in that particular region. Although the registries cover various parts of the country, they do not sufficiently cover or represent various regions which are far distant from the center of location of PBCR. Still, the NCRP reports are the only source of the cancer data, and no other sources are available for cancer statistics in India. Even though the PBCRs are spread throughout the country diversely, on the whole, the PBCRs cover only about 7% of the country's population. Achieving full coverage of a huge country such as India is practically not possible. India still has 7.45% coverage of total country's population for cancer estimation as compared to China, which has recently enhanced to 22% coverage of the population with 308 cancer registries in the year 2014 from 11% population coverage in the year 1998.[24] Thus, there is still scope for India to target for a higher number of registries to achieve further higher coverage of the population in cancer enumeration.
CONCLUSIONS
Proportion of tobacco-related proportion of Tobacco Related cancers out of all cancers was still high. Northeast region was at the highest risk of developing TRCs among all cancer registries in all the regions. Among all TRC sites, esophagus, lung, hypopharynx, and mouth were the leading cancer sites for both men and women. Number of cancer registries be enhanced across nation for additional adequate representation of all regions of nation. Effective interventions are needed to reduce the use of tobacco to reduce the burden of disease.
Financial support and sponsorship
Nil.