 PDF
PDF  Views
Views  Share
Share


A Prospective Study to Evaluate the Prevalence of Microsatellite Instability in Endometrial Carcinoma by using Immunohistochemistry for Mismatch Repair Proteins as a Surrogate Marker
CC BY 4.0 · Indian J Med Paediatr Oncol 2026; 47(03): 191-196
DOI: DOI: 10.1055/s-0043-1775853
Abstract
Introduction
Microsatellite instability (MSI), resulting from defects in the DNA mismatch repair (MMR) system, is one of the major molecular pathways involved in the pathogenesis of endometrial carcinoma. Immunohistochemistry (IHC) for MMR proteins serves as a practical and cost-effective method for identifying MSI and screening patients for Lynch syndrome.
Objectives
To determine the prevalence of MMR deficiency/MSI in endometrial carcinoma using immunohistochemistry and to correlate the findings with various histopathological parameters.
Materials and Methods
A total of 114 cases of endometrial carcinoma were evaluated. Immunohistochemical expression of the MMR proteins PMS2, MLH1, MSH2, and MSH6 was assessed using the Dako EnVision FLEX system on formalin-fixed, paraffin-embedded tumor tissue sections. The frequency and pattern of MMR protein loss were analyzed and correlated with histological subtypes.
Results
Among the 114 cases studied, the majority were endometrioid carcinomas (n = 93, 81.6%), followed by serous carcinomas (n = 12, 10.5%), carcinosarcomas (n = 5, 4.4%), dedifferentiated uterine carcinomas (n = 3, 2.6%), and clear cell carcinoma (n = 1, 0.9%). MMR deficiency was identified in 21 cases (18%). Of these, 20 cases were of the endometrioid subtype and 1 case was a dedifferentiated uterine carcinoma. Loss of MMR protein expression occurred in paired patterns, involving either PMS2/MLH1 or MSH2/MSH6.
Conclusion
MMR deficiency/MSI is present in a significant proportion of endometrial carcinomas, particularly those of the endometrioid subtype. Immunohistochemical evaluation of MMR proteins is a highly sensitive and cost-effective alternative to molecular MSI testing and serves as an effective screening tool for Lynch syndrome. Routine MMR testing should be offered to all patients with endometrial carcinoma.
Keywords
mismatch repair proteins - microsatellite instability - Lynch syndrome - endometrial cancer - uterine corpus cancerAuthor's Contributions
This article has been read and approved by all the authors.
Publication History
Article published online:
07 May 2024
© 2024. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
We recommend
- Study of Immunohistochemical Expression Patterns of Mismatch Repair Proteins in Endometrial Carcinoma and Endometrial Hyperplasia: An Institutional StudyBelani Vaishali Tulsidas, Kausalya Kumari Sahu, Ranjitha Rao, et al., TH Open, 2025
- Endometriosis-associated MalignancyN. Krawczyk, Journal of Pediatric Biochemistry, 2016
- Study of PTEN immunohistochemical expression in endometrial hyperplasiaSabuhi Qureshi, Asian Journal of Oncology, 2016
- Multiple primary cancer, including basal and squamous cell carcinomas of the skin with loss of mismatch-repair protein expression in a HNPCC family member – Cas...L. Czakó, Zeitschrift für Gastroenterologie, 2004
- MLH1 promoter hypermethylation in mismatch repair deficient endometrial cancer.Defining a new subgroup?N Pauly, Geburtshilfe und Frauenheilkunde, 2022
- Early identification and management of chronic kidney disease: summary of NICE guidanceEmily Crowe, David Halpin, Paul E. Stevens, The BMJ, 2008
- Genetic diversity of tumors with mismatch repair deficiency influences anti–PD-1 immunotherapy response<svg viewBox="0 0 24 24" fill="none" xmlns="http://www.w3.org/2000/svg">
</svg> Rajarsi Mandal, Science, 2019 - Advances in the management of endometrial cancerBradley R. Corr, Britt Erickson, Emma L. Barber, et al., The BMJ, 2025
- Identification of NFASC and CHL1 as Two Novel Hub Genes in Endometriosis Using Integrated Bioinformatic Analysis and Experimental VerificationPharmacogenomics & Personalized Medicine
- An alternative to the diagnostic dilatation and curettage--endometrial cytology.D. W. POLSON, Anne Morse, R. W. Beard, The BMJ, 1984
Abstract
Introduction
Microsatellite instability (MSI), resulting from defects in the DNA mismatch repair (MMR) system, is one of the major molecular pathways involved in the pathogenesis of endometrial carcinoma. Immunohistochemistry (IHC) for MMR proteins serves as a practical and cost-effective method for identifying MSI and screening patients for Lynch syndrome.
Objectives
To determine the prevalence of MMR deficiency/MSI in endometrial carcinoma using immunohistochemistry and to correlate the findings with various histopathological parameters.
Materials and Methods
A total of 114 cases of endometrial carcinoma were evaluated. Immunohistochemical expression of the MMR proteins PMS2, MLH1, MSH2, and MSH6 was assessed using the Dako EnVision FLEX system on formalin-fixed, paraffin-embedded tumor tissue sections. The frequency and pattern of MMR protein loss were analyzed and correlated with histological subtypes.
Results
Among the 114 cases studied, the majority were endometrioid carcinomas (n = 93, 81.6%), followed by serous carcinomas (n = 12, 10.5%), carcinosarcomas (n = 5, 4.4%), dedifferentiated uterine carcinomas (n = 3, 2.6%), and clear cell carcinoma (n = 1, 0.9%). MMR deficiency was identified in 21 cases (18%). Of these, 20 cases were of the endometrioid subtype and 1 case was a dedifferentiated uterine carcinoma. Loss of MMR protein expression occurred in paired patterns, involving either PMS2/MLH1 or MSH2/MSH6.
Conclusion
MMR deficiency/MSI is present in a significant proportion of endometrial carcinomas, particularly those of the endometrioid subtype. Immunohistochemical evaluation of MMR proteins is a highly sensitive and cost-effective alternative to molecular MSI testing and serves as an effective screening tool for Lynch syndrome. Routine MMR testing should be offered to all patients with endometrial carcinoma.
Keywords
Introduction
With 417,367 (2.2%, of all cancer cases) new cases diagnosed globally in 2020 and 97,370 recorded deaths, endometrial cancer is the sixth most common cancer in women.[1] In India, endometrioid cancer is the 22nd most commonly detected malignancy, with approximately 16,413 new cases (1.2%) reported in 2020, according to Globocan data.[2] It is among the five most common malignancies detected in females in the Indian population.[3]
According to the World Health Organization classification, endometrial carcinomas can be histologically classified as endometrioid carcinoma, serous carcinoma, clear cell carcinoma, undifferentiated and dedifferentiated carcinomas, carcinosarcomas, and others.[4] Recent advancements in our understanding of the molecular biology of tumor cells have led to the advocacy for the inclusion of molecular characteristics in both the classification and risk stratification of Endometrial Carcinoma (EC). This is because molecular characteristics can provide a more accurate understanding of the biological behavior of a patient's disease, which can lead to improved treatment decisions. In a seminal paper published by The Cancer Genome Atlas (TCGA) in 2013, it classified endometrial cancers into four major genomic subtypes: (1) POLE (DNA polymerase ε) ultramutated, (2) hypermutated/microsatellite unstable (microsatellite instability [MSI]), (3) copy number low/microsatellite stable group, and (4) copy number high (serous-like) group.[5]
Numerous genes linked to cancer have been examined in endometrial carcinoma, of which the molecular phenotype known as MSI has drawn a lot of focus. Endometrial cancer is the most common cancer known to be associated with MSI after colorectal cancer.[6] MSI is the accumulation of mismatches, insertions, and deletions in repeated nucleotide sequences due to defects in DNA mismatch repair (MMR). MMR is a crucial cellular defense system that rectifies any DNA alterations produced during DNA replication. MSI is the hallmark of a defective MMR system. DNA MMR system in patients that display MSI can be inactivated either by (1) germline mutations found in Lynch syndrome amounting to 2 to 3%, of endometrial cancers or (2) somatic promoter hypermethylation and silencing of MLH1 observed in 20%, of sporadic endometrial cancers.[7] [8] [9] Regardless of the underlying mechanism, the inactivation of the DNA MMR system leads to an increased mutation rate, which contributes to tumorigenesis. The majority of MSI in endometrial and colorectal cancers is caused by defects in DNA MMR genes, mainly MLH1, MSH2, MSH6, and PMS2.[9] Loss of function of MMR protein MLH1 due to methylation of the MLH1 gene promoter, seen more commonly in sporadic tumors, and thus also loss of its binding partner PMS2, can be detected as a loss of expression of these proteins by immunohistochemical (IHC).[10]
As per the recommendations of National Comprehensive Cancer Network, all newly diagnosed ECs patients should be tested for loss of MMR function via IHC and/or MSI analysis independent of the clinical criteria.[11] IHC screening for MMR proteins is a relatively affordable alternative and can guarantee sensitivity and specificity at the same time. MMR proteins exist in heterodimers viz, PMS2 dimerizes with MLH1 and MSH2 dimerizes with MSH6. This explains the concurrent loss of either PMS2 and MLH1 or MSH2 and MSH6 in ECs.[12]
The tumors with MSI have a high incidence of somatic mutations that results in the production of proteins with new immunogenicity. The host immune system responds to these new antigens by excessive peritumoral T-cell infiltration.[13] Cancer cells circumvent the host immunological response by activating pathways that inhibit T-cell activation (cytotoxic T-lymphocyte–associated antigen and programmed cell death ligand 1).[14] This principle forms the basis for the use of immune checkpoint inhibitors as potential therapeutic agents in tumors with MSI. A phase 2 study was conducted by Le et al to evaluate the clinical activity of the anti-PD 1 drug, pembrolizumab, in tumors with MMR that included colorectal as well as noncolorectal tumors demonstrated the importance of MMR status in predicting the clinical benefit of immune checkpoint blockade with pembrolizumab.[15]
Dostarlimab, an anti-PD 1 drug, was used singularly by Cercek et al to treat MMR-deficient (dMMR), locally progressed rectal cancer. They observed that this tumor was extremely sensitive to PD 1 inhibition.[16] Thus, MSI analysis is also a predictive biomarker for the therapeutic efficacy of anti-PD ligand antibodies.[13] According to the College of American Pathologists guidelines for MMR and MSI testing, which were recently endorsed by the American Society of Clinical Oncology, immunohistochemistry for MMR proteins is preferred over MSI testing by polymerase chain reaction or next-generation sequencing for the identification of DNA MMR defects in patients with endometrial cancer who are being considered for immune checkpoint inhibitors.[17]
In this study, we evaluated the endometrial cancers for their expression of MMR proteins by IHC and correlated their MMR status with age and various histopathological parameters.
Materials and Methods
This study was conducted in a tertiary hospital in western part of India between June 2018 and June 2020 to survey the prevalence of MMR protein deficiency using immunohistochemistry in the hysterectomy specimens of endometrial cancers. The patient data were obtained from the electronic database of the hospital records as well as the departmental register of histopathological specimens received in the lab. This study included only the cases for which a complete assessment of pathological parameters and staging was available. In addition, cases that had received presurgical neoadjuvant therapy were excluded from this study
Immunohistochemistry testing for the four MMR proteins: MSH2 (clone FE11), MSH6 (clone EP49), PMS2 (clone EP51), and MLH1 (clone ES05) was done on 114 endometrial cancer cases. Testing was done on the endometrial cancer tumor tissue paraffin blocks of hysterectomy specimens using the Dako EnVision FLEX system. The complete absence of nuclear staining with a positive internal control was considered a loss of nuclear expression of an MMR protein. Tumor with loss of nuclear expression of any MMR protein was regarded as dMMR; tumor cells with intact nuclear expression of all four MMR proteins were regarded as MMR-proficient ([Fig. 1]).
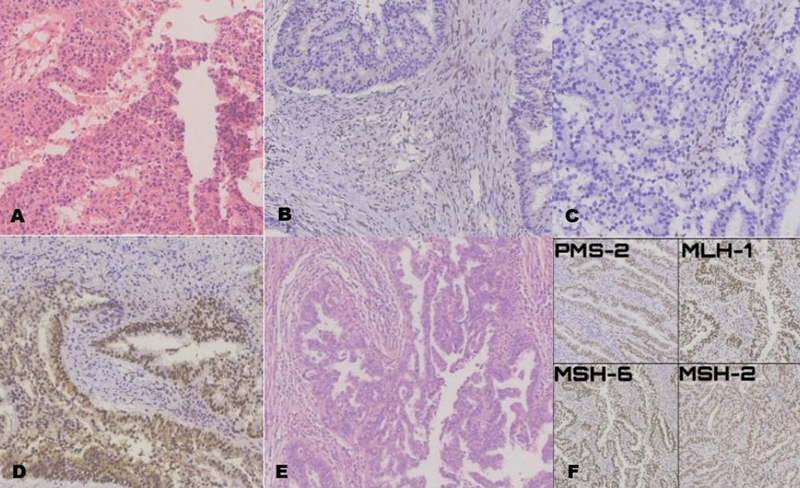
Fig 1: RISMA flow diagram illustrating the study selection process for the systematic review.
The sample size was calculated using formula: n = p (1 − p) [(zα + z1 − β)/(p − p0)]2, where n is the sample size, p = 0.52 (52%, prevalence of MSI-H in endometrial cancer patients), α is Type I error = 5%; zα = 1.96 two-sided, zα = 1.64 one-sided, β is Type II error, 1 − β is power; z1–β = 0.84 for 1–β = 80%, effect size = (p − p0) = ± 0.13 (13%).
Statistical Package for the Social Sciences (SPSS Inc. 233, Chicago, Illinois, United States) software was used for statistical analysis. Unpaired Student's t-test was used for quantitative data and a χ2 test was used for categorical variables with more than two; p-values from Fisher's exact test are presented where appropriate due to small counts.
This study was reviewed and approved by the Institutional Ethical Committee at the meeting held on December 28, 2018 (Number: DNB_2018_PATH_005) and adhered to the tenets of the Declaration of Helsinki. The patient's consent was waived by the Institutional Committee.
Results
The findings of our study, which analyzed 114 endometrial cancer specimens for expression of MMR proteins and its relationship to various histopathological parameters and age, are summarized in [Table 1]. The average age of the study population was 62 years (range: 36–91 years). Among these, 9 patients were less than or equal to 50 years of age at the time of diagnosis, whereas the rest were more than 50 years old. A strong correlation was found between dMMR and age greater than 50 years (p = 0.016). On histologic subtyping, endometrioid carcinoma accounted for the majority of cases (93 cases, 81.6%). These tumors were graded as per the International Federation of Gynecology and Obstetrics (FIGO) criteria. Nonendometrioid carcinomas, except for mucinous carcinomas, are conventionally considered high grade. Out of the 93 endometrioid cancer cases found, 69 were Grade 1, 16 were Grade 2, and 8 were Grade 3.
|
Number of cases (%) |
Retained expression of all markers |
Loss of MLH1/PMS2 expression |
Loss of MSH2/MSH6 expression |
Total |
p-Value |
|---|---|---|---|---|---|
|
Histology diagnosis |
|||||
|
Endometrioid carcinoma |
73 (78.5%) |
19 (20.43%) |
1 (1.07%) |
93 |
|
|
Serous carcinoma |
12 (100%) |
0 |
0 |
12 |
0.737 |
|
Clear cell carcinoma |
1 (100%) |
0 |
0 |
1 |
|
|
MMMT |
5 (100%) |
0 |
0 |
5 |
|
|
DDUC |
2 (66.67%) |
1 (33.33%) |
0 |
3 |
|
|
FIGO stage |
|||||
|
IA |
38 (77.55%) |
11 (22.45%) |
0 |
49 |
0.094 |
|
IB |
31 (88.57%) |
4 (11.43%) |
0 |
35 |
|
|
II |
13 (86.67%) |
2 (13.33%) |
0 |
15 |
|
|
IIIA |
5 (100%) |
0 |
0 |
5 |
|
|
IIIB |
1 (50%) |
1 (50%) |
0 |
2 |
|
|
IIIC1 |
2 (50%) |
2 (50%) |
1 |
5 |
|
|
IVB |
3 (100%) |
0 |
0 |
3 |
|
|
Grade |
|||||
|
G1 |
58 (84.06%) |
11 (15.94%) |
0 |
69 |
|
|
G2 |
11 (68.75%) |
4 (25%) |
1 (6.25%) |
16 |
0.071 |
|
G3 |
6 (60%) |
4 (40%) |
0 |
10 |
|
|
High |
18 (94.73%) |
1 (5.27%) |
0 |
19 |
|
|
Myometrial invasion |
|||||
|
< 1/2 or absent |
45 (77.58%) |
12 (20.69%) |
1 (1.72%) |
58 |
0.388 |
|
≥1/2 |
48 (85.71%) |
8 (14.28%) |
0 |
56 |
|
|
Age (y) |
|||||
|
≤50 |
9 (69.23%) |
3 (23.07%) |
1 (7.7%) |
13 |
0.016 |
|
> 50 |
84 (83.17%) |
17 (16.83%) |
0 |
101 |
|
On IHC analysis for MMR proteins, it was found that 21 out of 114 cases (18.4%) of endometrial cancers were deficient for MMR proteins (95%, confidence interval [CI], 11.3–25.5%).
Twenty cases had a combined loss of PMS2 and MLH1, whereas only one case had a combined loss of MSH2 and MSH6. Tumors with a loss of only one MMR protein were not present in our study. Furthermore, the histologic subtypes of endometrioid cancer (n = 20) and dedifferentiated uterine carcinoma (n = 1) accounted for all the dMMR cases. The prevalence of MMR deficiency in endometrioid carcinomas was 21.3%, with a 95% CI of 13.8 to 28.8%.
Eighty-five cases of low FIGO grade (Grades 1 and 2) endometrioid carcinoma made up our study, whereas 29 cases were high grade, which combined both endometrioid (n = 10) and nonendometrioid carcinoma (n = 19). A total of 16 low-grade and 5 high-grade cases with deficient MMR expression were identified.
Tumor invasion into greater than or equal to half the myometrium was identified in 56 cases, of which 8 cases showed deficient MMR expression. Tumors having less than half or absence of invasion comprised 45 cases, of which 13 cases showed deficient MMR expression. We could not establish any statistically significant relation between myometrial invasion and MMR expression.
Subsequently, as per FIGO staging classification, 43%, of the cases were stage group IA (pT1a), 30.7% were stage IB (pT1b), 13.2%, cases were stage group II (pT2), 4.4%, were stage IIIA (pT3a), 1.8%, were stage IIIB (pT3b), and 2.6%, cases were stage group IVB (pM1). Only four of the 21 patients with deficient MMR expression were stage III or higher at the time of diagnosis. We did not find any statistically significant association between dMMR protein expression and tumor stage group, myometrial invasion, histologic grade, or morphological subtype.
Discussion
The MSI phenotype continues to serve as the hallmark of defective MMR. This is because germline mutations in MLH1, MSH2, MSH6, and PMS2 are responsible for genetic susceptibility to colorectal cancer known as Lynch syndrome or hereditary nonpolyposis colorectal cancer.[18]
The role of MSI as a marker for favorable prognosis has been very well established in colorectal cancers. However, its role in endometrial cancers is yet to be ascertained. A meta-analysis done by Raffone et al found that MSI is an unfavorable prognostic factor in early-stage EC, which otherwise has a good prognosis. Paradoxically, MSI is an advantageous prognostic factor in high-risk carcinomas, which typically have a poor prognosis.[19]
In our study, the prevalence of MMR proteins deficiency was found in 18%, (21 out of 114) cases of endometrial cancers. Twenty cases showed a concurrent loss of PMS2 and MLH1, whereas only one case showed a concurrent loss of MSH2 and MSH6. The prevalence of MMR deficiency ranged from 15 to 30%, in various other studies.[19] [20] [21] [22] The majority of our cases (20 out of 21) with deficient MMR proteins were of endometrioid carcinoma (20 cases) on histologic subtyping, of which 19 cases were deficient for PMS2 and MLH1, whereas only 1 case showed deficient expression of MSH2 and MSH6. A single case of dedifferentiated carcinoma was deficient for MMR proteins. Other studies conducted showed a statistically significant association between MMR deficiency and endometrioid and dedifferentiated/undifferentiated uterine carcinomas.[20] [21] [23] Although we had similar observations, we could not establish statistically significant conclusions (p = 0.737) as the number of nonendometrioid cancers was less. We found no association between the grade of tumor and MMR status, which is similar to other studies.[19] [20] [21] We were unable to establish any statistically significant association between myometrial invasion and MMR deficiency, which has been reported in a few studies.[20] [21] This difference in results could be due to a small sample size.
A comprehensive review and meta-analysis by Raffone et al examined the diagnostic precision of MMR proteins IHC as a stand-in for molecular testing for MSI in endometrial malignancies, as well as the possibility of using a panel of just two MMR proteins to further reduce costs. They found IHC for MMR proteins to be a highly reliable substitute for MSI molecular testing (sensitivity of 0.96 and specificity of 0.95) in endometrial cancer. They further proposed that the combination of MSH6 and PMS2 may help to reduce costs while maintaining diagnostic accuracy.[19]
Talhouk et al designed a molecular categorization system—Proactive Molecular Risk Classifier for Endometrial Cancer—based on the TCGA molecular subcategories and tested its practicality and prognostic potential in ECs using immunohistochemistry for the MMR and P53 proteins and POLE sequencing. Four prognostic subgroups were identified: dMMR, POLE, p53 Wild Type (wt), and p53 Null/Missense Mutations (abn), each of which had unique overall, disease-specific, and progression-free survival rates. The most promising outcome was seen in tumors with POLE exonuclease domain mutations, and the worst prognosis was seen in tumors with p53 abn.[24] Such studies are required in the Indian population to assess biological behavior and to improve clinical management and outcomes. The advantages of IHC for MMR include its simplicity, availability, and relatively lower cost compared with molecular testing. Patterns of loss of MMR proteins can further help in guiding the reflex molecular testing for MSI.[19]
The disadvantages of IHC for MMR proteins include interobserver variation in interpretation especially in cases with heterogeneous staining patterns and false negativity (production of nonfunctional protein which stains with MMR IHC).[19] [25]
Limitations
Clinical follow-up of the patients and its correlation with MSI status was not assessed.
Recommendations
A larger study with longer follow-up will help to confirm the relationship between the histology of endometrial carcinomas and MSI status.
Conclusion
MSI is one of the major molecular pathways contributing to tumorigenesis in endometrial carcinomas. Immunohistochemistry for MMR proteins is a highly sensitive and cost-effective alternative for molecular testing for MSI. It is also a tool for screening patients for Lynch syndrome. IHC testing for MMR should be offered to all patients of endometrial cancers.
Conflict of Interest
None declared.
Acknowledgments
The authors would like to specially acknowledge Dr. Deepa Puntambekar for the initial conceptualization, Dr. Asawari Kanade for statistical analysis, and Sucheta Nirmal, Meenal Khire, Sushma Ingale, Snehal Marne, and Shivaji Darekar for technical assistance.
Author's Contributions
This article has been read and approved by all the authors.
References
- Sung H, Ferlay J, Siegel RL. et al. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021; 71 (03) 209-249
- https://gco.iarc.fr/today/online-analysis-table?v=2020&mode=cancer&mode_population=continents&population=900&populations=356&key=asr&sex=2&cancer=39&type=0&statistic=5&prevalence=0&population_group=0&ages_group[]=0&ages_group[]=17&group_cancer=1&include_nmsc=0&include_nmsc_other=1#collapse-by_country
- Mathur P, Sathishkumar K, Chaturvedi M. et al; ICMR-NCDIR-NCRP Investigator Group. Cancer Statistics, 2020: report from National Cancer Registry Programme, India. JCO Glob Oncol 2020; 6: 1063-1075
- International Agency for Research on Cancer, World Health Organization. WHO Classification of Female Genital Tumors: Who Classification of Tumors. 5th ed. (WHO Classification of Tumors Editorial Board, ed.). IARC; 2020
- Kandoth C, Schultz N, Cherniack AD. et al; Cancer Genome Atlas Research Network. Integrated genomic characterization of endometrial carcinoma. Nature 2013; 497 (7447) 67-73 [published correction appears in Nature. 2013;500(7461):242]
- Win AK, Lindor NM, Young JP. et al. Risks of primary extracolonic cancers following colorectal cancer in lynch syndrome. J Natl Cancer Inst 2012; 104 (18) 1363-1372
- Buecher B, De Pauw A, Bazire L. et al. Sporadic endometrial adenocarcinoma with MMR deficiency due to biallelic MSH2 somatic mutations. Fam Cancer 2018; 17 (02) 281-285
- Kahn RM, Gordhandas S, Maddy BP. et al. Universal endometrial cancer tumor typing: how much has immunohistochemistry, microsatellite instability, and MLH1 methylation improved the diagnosis of Lynch syndrome across the population?. Cancer 2019; 125 (18) 3172-3183
- Kurman RJ, Ellenson LH, Ronnett BM. Blaustein's Pathology of the Female Genital Tract. Springer;; 2011
- Ligtenberg MJ, Kuiper RP, Chan TL. et al. Heritable somatic methylation and inactivation of MSH2 in families with Lynch syndrome due to deletion of the 3′ exons of TACSTD1. Nat Genet 2009; 41 (01) 112-117
- Nccn.org. . Accessed June 26, 2022 at: https://www.nccn.org/professionals/physician_gls/pdf/uterine_blocks.pdf
- Mojtahed A, Schrijver I, Ford JM, Longacre TA, Pai RK. A two-antibody mismatch repair protein immunohistochemistry screening approach for colorectal carcinomas, skin sebaceous tumors, and gynecologic tract carcinomas. Mod Pathol 2011; 24 (07) 1004-1014
- Kunitomi H, Banno K, Yanokura M. et al. New use of microsatellite instability analysis in endometrial cancer. Oncol Lett 2017; 14 (03) 3297-3301
- Kumar V, Abbas AK, Aster J. Robbins & Cotran Pathologic Basis of Disease E-Book. 10th ed. Elsevier;; 2020
- Le DT, Uram JN, Wang H. et al. PD-1 blockade in tumors with mismatch-repair deficiency. N Engl J Med 2015; 372 (26) 2509-2520
- Cercek A, Lumish M, Sinopoli J. et al. PD-1 blockade in mismatch repair-deficient, locally advanced rectal cancer. N Engl J Med 2022; 386 (25) 2363-2376
- Vikas P, Messersmith H, Compton C. et al. Mismatch repair and microsatellite instability testing for immune checkpoint inhibitor therapy: ASCO endorsement of College of American Pathologists guideline. J Clin Oncol 2023; 41 (10) 1943-1948
- Hendriks YM, de Jong AE, Morreau H. et al. Diagnostic approach and management of Lynch syndrome (hereditary nonpolyposis colorectal carcinoma): a guide for clinicians. CA Cancer J Clin 2006; 56 (04) 213-225
- Raffone A, Travaglino A, Cerbone M. et al. Diagnostic accuracy of immunohistochemistry for mismatch repair proteins as surrogate of microsatellite instability molecular testing in endometrial cancer. Pathol Oncol Res 2020; 26 (03) 1417-1427
- Black D, Soslow RA, Levine DA. et al. Clinicopathologic significance of defective DNA mismatch repair in endometrial carcinoma. J Clin Oncol 2006; 24 (11) 1745-1753
- Kanopienė D, Smailytė G, Vidugirienė J, Bacher J. Impact of microsatellite instability on survival of endometrial cancer patients. Medicina (Kaunas) 2014; 50 (04) 216-221
-
Basil JB, Goodfellow PJ, Rader JS, Mutch DG, Herzog TJ. Clinical significance of microsatellite instability in endometrial carcinoma. Cancer 2000; 89 (08) 1758-1764 3.0.CO;2-A" target="linkout" data-target="CrossRef" data-id="CrossRef" data-url="https://doi.org/10.1002/1097-0142(20001015)89:8<1758>3.0.CO;2-A" style="color: rgb(1, 52, 118); outline-width: 0px; outline-color: transparent !important; padding-right: 10px;">Crossref PubMed Search in Google ScholarDownload RIS citation
- Broaddus RR, Lynch HT, Chen LM. et al. Pathologic features of endometrial carcinoma associated with HNPCC: a comparison with sporadic endometrial carcinoma. Cancer 2006; 106 (01) 87-94
- Talhouk A, McConechy MK, Leung S. et al. Confirmation of ProMisE: a simple, genomics-based clinical classifier for endometrial cancer. Cancer 2017; 123 (05) 802-813
- Bruegl AS, Ring KL, Daniels M, Fellman BM, Urbauer DL, Broaddus RR. Clinical challenges associated with universal screening for Lynch syndrome-associated endometrial cancer. Cancer Prev Res (Phila) 2017; 10 (02) 108-115
Address for correspondence
Publication History
Article published online:
07 May 2024
© 2024. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
We recommend
- Study of Immunohistochemical Expression Patterns of Mismatch Repair Proteins in Endometrial Carcinoma and Endometrial Hyperplasia: An Institutional StudyBelani Vaishali Tulsidas, Kausalya Kumari Sahu, Ranjitha Rao, et al., TH Open, 2025
- Endometriosis-associated MalignancyN. Krawczyk, Journal of Pediatric Biochemistry, 2016
- Study of PTEN immunohistochemical expression in endometrial hyperplasiaSabuhi Qureshi, Asian Journal of Oncology, 2016
- Multiple primary cancer, including basal and squamous cell carcinomas of the skin with loss of mismatch-repair protein expression in a HNPCC family member – Cas...L. Czakó, Zeitschrift für Gastroenterologie, 2004
- MLH1 promoter hypermethylation in mismatch repair deficient endometrial cancer.Defining a new subgroup?N Pauly, Geburtshilfe und Frauenheilkunde, 2022
- Differential Proteomics Analysis of Endometriosis in Blood Stasis SyndromeChinese Journal of Integrative Medicine
- Bioinformatic Analysis of Key Genes of Endometriosis and Traditional Chinese Medicine in the Related TherapiesGU Fengqun, LI Weihong, NING Min, et al., Western Journal of Traditional Chinese Medicine, 2023
- Effects of Curcumin Regulating Yes-Associated Protein 1 on Warburg Effect and Biological Behaviors of Patients with Endometrial Carcinoma<svg viewBox="0 0 24 24" fill="none" xmlns="http://www.w3.org/2000/svg">
</svg> Yanxia Hu, Xiaoxia Song, Xihong Zhang, Journal of new Chinese medicine, 2024 - Study on Mechanism of Shengjiang Longlian Decoction(升降龙莲汤) in the Treatment of Endometrial cancer Based on Network Pharmacology,GEO database and Molecular Docki...Xinxin Wang, Haifeng YUN, Chunbo Jiang, et al., Journal of practical traditional Chinese internal medicine, 2024
- Clinical Study on Hongjin Xiaojie Capsules Combined with Leuprorelin Acetate for Endometriosis<svg viewBox="0 0 24 24" fill="none" xmlns="http://www.w3.org/2000/svg">
</svg> Xiaoling Yu, Jing'an XU, Rongrong Chen, Journal of new Chinese medicine, 2024
Fig 1: RISMA flow diagram illustrating the study selection process for the systematic review.
References
- Sung H, Ferlay J, Siegel RL. et al. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021; 71 (03) 209-249
- https://gco.iarc.fr/today/online-analysis-table?v=2020&mode=cancer&mode_population=continents&population=900&populations=356&key=asr&sex=2&cancer=39&type=0&statistic=5&prevalence=0&population_group=0&ages_group[]=0&ages_group[]=17&group_cancer=1&include_nmsc=0&include_nmsc_other=1#collapse-by_country
- Mathur P, Sathishkumar K, Chaturvedi M. et al; ICMR-NCDIR-NCRP Investigator Group. Cancer Statistics, 2020: report from National Cancer Registry Programme, India. JCO Glob Oncol 2020; 6: 1063-1075
- International Agency for Research on Cancer, World Health Organization. WHO Classification of Female Genital Tumors: Who Classification of Tumors. 5th ed. (WHO Classification of Tumors Editorial Board, ed.). IARC; 2020
- Kandoth C, Schultz N, Cherniack AD. et al; Cancer Genome Atlas Research Network. Integrated genomic characterization of endometrial carcinoma. Nature 2013; 497 (7447) 67-73 [published correction appears in Nature. 2013;500(7461):242]
- Win AK, Lindor NM, Young JP. et al. Risks of primary extracolonic cancers following colorectal cancer in lynch syndrome. J Natl Cancer Inst 2012; 104 (18) 1363-1372
- Buecher B, De Pauw A, Bazire L. et al. Sporadic endometrial adenocarcinoma with MMR deficiency due to biallelic MSH2 somatic mutations. Fam Cancer 2018; 17 (02) 281-285
- Kahn RM, Gordhandas S, Maddy BP. et al. Universal endometrial cancer tumor typing: how much has immunohistochemistry, microsatellite instability, and MLH1 methylation improved the diagnosis of Lynch syndrome across the population?. Cancer 2019; 125 (18) 3172-3183
- Kurman RJ, Ellenson LH, Ronnett BM. Blaustein's Pathology of the Female Genital Tract. Springer;; 2011
- Ligtenberg MJ, Kuiper RP, Chan TL. et al. Heritable somatic methylation and inactivation of MSH2 in families with Lynch syndrome due to deletion of the 3′ exons of TACSTD1. Nat Genet 2009; 41 (01) 112-117
- Nccn.org. . Accessed June 26, 2022 at: https://www.nccn.org/professionals/physician_gls/pdf/uterine_blocks.pdf
- Mojtahed A, Schrijver I, Ford JM, Longacre TA, Pai RK. A two-antibody mismatch repair protein immunohistochemistry screening approach for colorectal carcinomas, skin sebaceous tumors, and gynecologic tract carcinomas. Mod Pathol 2011; 24 (07) 1004-1014
- Kunitomi H, Banno K, Yanokura M. et al. New use of microsatellite instability analysis in endometrial cancer. Oncol Lett 2017; 14 (03) 3297-3301
- Kumar V, Abbas AK, Aster J. Robbins & Cotran Pathologic Basis of Disease E-Book. 10th ed. Elsevier;; 2020
- Le DT, Uram JN, Wang H. et al. PD-1 blockade in tumors with mismatch-repair deficiency. N Engl J Med 2015; 372 (26) 2509-2520
- Cercek A, Lumish M, Sinopoli J. et al. PD-1 blockade in mismatch repair-deficient, locally advanced rectal cancer. N Engl J Med 2022; 386 (25) 2363-2376
- Vikas P, Messersmith H, Compton C. et al. Mismatch repair and microsatellite instability testing for immune checkpoint inhibitor therapy: ASCO endorsement of College of American Pathologists guideline. J Clin Oncol 2023; 41 (10) 1943-1948
- Hendriks YM, de Jong AE, Morreau H. et al. Diagnostic approach and management of Lynch syndrome (hereditary nonpolyposis colorectal carcinoma): a guide for clinicians. CA Cancer J Clin 2006; 56 (04) 213-225
- Raffone A, Travaglino A, Cerbone M. et al. Diagnostic accuracy of immunohistochemistry for mismatch repair proteins as surrogate of microsatellite instability molecular testing in endometrial cancer. Pathol Oncol Res 2020; 26 (03) 1417-1427
- Black D, Soslow RA, Levine DA. et al. Clinicopathologic significance of defective DNA mismatch repair in endometrial carcinoma. J Clin Oncol 2006; 24 (11) 1745-1753
- Kanopienė D, Smailytė G, Vidugirienė J, Bacher J. Impact of microsatellite instability on survival of endometrial cancer patients. Medicina (Kaunas) 2014; 50 (04) 216-221
-
Basil JB, Goodfellow PJ, Rader JS, Mutch DG, Herzog TJ. Clinical significance of microsatellite instability in endometrial carcinoma. Cancer 2000; 89 (08) 1758-1764 3.0.CO;2-A" target="linkout" data-target="CrossRef" data-id="CrossRef" data-url="https://doi.org/10.1002/1097-0142(20001015)89:8<1758>3.0.CO;2-A" style="color: rgb(1, 52, 118); outline-width: 0px; outline-color: transparent !important; padding-right: 10px;">Crossref PubMed Search in Google ScholarDownload RIS citation
- Broaddus RR, Lynch HT, Chen LM. et al. Pathologic features of endometrial carcinoma associated with HNPCC: a comparison with sporadic endometrial carcinoma. Cancer 2006; 106 (01) 87-94
- Talhouk A, McConechy MK, Leung S. et al. Confirmation of ProMisE: a simple, genomics-based clinical classifier for endometrial cancer. Cancer 2017; 123 (05) 802-813
- Bruegl AS, Ring KL, Daniels M, Fellman BM, Urbauer DL, Broaddus RR. Clinical challenges associated with universal screening for Lynch syndrome-associated endometrial cancer. Cancer Prev Res (Phila) 2017; 10 (02) 108-115