 PDF
PDF  Views
Views  Share
Share


A rare case of lung cancer presenting as an ischioanal fossa mass
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2016; 37(04): 300-302
DOI: DOI: 10.4103/0971-5851.195743
Abstract
Lung cancer metastasis commonly involves the adrenal glands, liver, bone, and brain. However, it can have some rarer forms of metastatic presentation making diagnosis difficult, especially in nonsmokers. We describe a rare case of lung cancer with metastasis to the ischioanal fossa. Overall, this case emphasizes that consideration should be given to wide range of diagnosis in atypical cases of anorectal masses. Lung cancer presenting as an ischioanal mass is not reported so far.
Publication History
Article published online:
12 July 2021
© 2016. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Abstract
Lung cancer metastasis commonly involves the adrenal glands, liver, bone, and brain. However, it can have some rarer forms of metastatic presentation making diagnosis difficult, especially in nonsmokers. We describe a rare case of lung cancer with metastasis to the ischioanal fossa. Overall, this case emphasizes that consideration should be given to wide range of diagnosis in atypical cases of anorectal masses. Lung cancer presenting as an ischioanal mass is not reported so far.
INTRODUCTION
Lung cancer is one of the most frequent and commonly diagnosed cancers worldwide, with a high mortality rate.[1] The most common sites for distant metastases of lung cancer are adrenal glands, liver, brain, and bone.[2,3] We present a case of a 75-year-old nonsmoker male who presented with an ischioanal mass. The biopsy showed adenocarcinoma without any colorectal mucosal lesion, which prompted a positron emission tomography (PET) computed tomography (CT) scan evaluation, leading to the diagnosis of Stage 4 lung cancer with metastasis to the ischioanal fossa and adrenal glands.
CASE REPORT
A 75-year-old male, nonsmoker, diabetic, hypertensive, postcoronary bypass was referred to our hospital with complaints of burning sensation in perianal area with a mass-like sensation causing hindrance to sit. There was no history of constipation, bleeding per-rectum, pain or mass per-abdomen or weight loss. On examination, a hard mass was felt on the external side around the perianal region. Per-rectum revealed a growth on the left lateral part around the anal region, no growth felt in the rectal mucosa, and the upper extent of the tumor could not be delineated. There was no other palpable mass or peripheral lymphadenopathy. Other systemic examination was normal. Contrast-enhanced CT of the abdomen and pelvis done outside showed a 3.7 cm × 4.2 cm × 2.8 cm mass in the perianal region, medially extending up to the external sphincter close to the anal verge. The mass was free from the prostate. The patient had undergone a biopsy from the mass outside, which was suggestive of moderately differentiated adenocarcinoma. No immunochemical (IHC) evaluation was done. With a suspicion of a skip lesion from a higher growth, we performed a sigmoido-colonoscopy which showed a hard mass on the left side of perianal region with no clear growth arising from the rectal or anal mucosa. Carcinoembryonic antigen was 205.7 ng/ml. In view of unusual site of adenocarcinoma in the perianal region, a PET/CT scan was done which revealed a 2.6 cm × 2.3 cm mass in the right lower lobe of lung with hilar and axillary lymphadenopathy, bilateral lung nodules with a small adrenal nodule along with a 4.8 cm × 3.5 cm mass in the left ischioanal fossa [Figures [Figures11 and and2].2]. We finally concluded that the patient has Stage 4 adenocarcinoma lung with metastases to ischioanal fossa, bilateral lung, and adrenal gland. Epidermal growth factor receptor (EGFR) and anaplastic lymphoma kinase (ALK) mutation analyses were negative. The patient was started on pemetrexed-carboplatin chemotherapy. After two cycles of pemetrexed-carboplatin, the patient did not have any benefit. Hence, subsequently, his chemotherapy was changed to paclitaxel-carboplatin and after the first cycle itself the mass began to shrink.
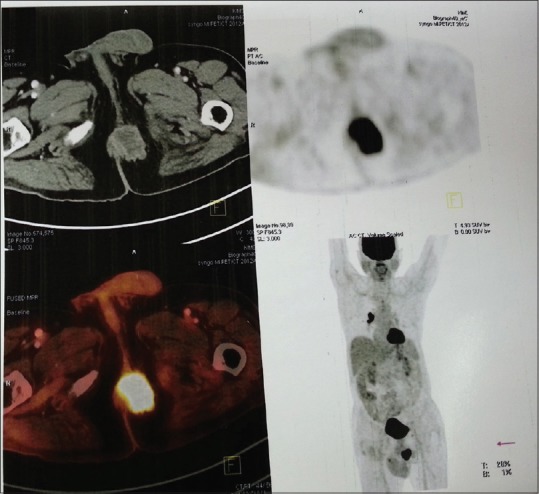
| Fig. 1 Positron emission tomography computed tomography showing fluorodeoxyglucose avid lesion in the ischioanal fossa
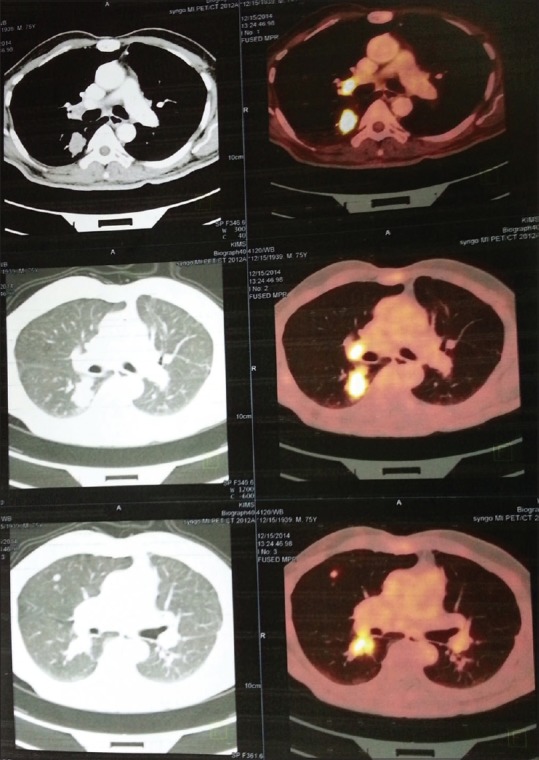
| Fig. 2 Positron emission tomography computed tomography showing fluorodeoxyglucose avid lung primary
DISCUSSION
Here, we present a case of lung adenocarcinoma with a rare presentation of an ischioanal mass in a nonsmoker which was diagnosed on PET/CT. Lung cancer metastases commonly involve the adrenal glands, bone, and brain.[4] Some rare sites of metastasis published in the literature are subcutaneous nodules, thyroid gland, intracranial tumor-meningioma, and multiple cavitary lesions in a patient with wild-type EGFR.[4,5,6,7] Primary neoplasms occurring in the ischiorectal fossa are very uncommon. Angiomyxoma is a rare neoplasm which can also present with a well-defined lobulated mass in the ischiorectal fossa as in our case.[8]
Lung cancer is generally believed to be smoker's disease as compared to nonsmoker's which many at times leads to delayed diagnosis in nonsmokers. In our patient, detailed imaging excluded primary origin in the abdominal cavity as well as from epithelial lining of the rectal and anal mucosa. The histopathology report suggested moderately differentiated adenocarcinoma which led to the suspicion of skip lesion, and later on, PET scan was done which showed the origin in the lung with metastasis to adrenal too. It is essential to distinguish pulmonary adenocarcinoma with intestinal differentiation from metastatic colorectal carcinoma because of critical differences in therapeutic strategies and prognosis, which can be done by IHC and EGFR analysis.[9]
EGFR mutations seem to influence the site of metastasis with a positive EGFR status favoring pleural metastasis in pulmonary adenocarcinoma.[10,11] Since EGFR and AKL mutation were found to be negative in our case, the treatment was started on pemetrexed (folate antagonist)-carboplatin chemotherapy and later on shifted to paclitaxel-carboplatin therapy which showed more effectiveness in suppressing the mass.
Overall, this case emphasizes that consideration should be given to wide range of diagnosis in atypical cases of anorectal masses. There are no similar reported cases of primary lung adenocarcinoma presenting as ischioanal fossa mass and this case represents a challenge in both diagnosis and long-term management.
CONCLUSION
There are no case reports of lung cancer presenting as an ischioanal fossa mass as the initial presentation. This case report emphasizes the varied forms of lung cancer presentation which is a diagnostic challenge, especially in nonsmokers.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
| Fig. 1 Positron emission tomography computed tomography showing fluorodeoxyglucose avid lesion in the ischioanal fossa
| Fig. 2 Positron emission tomography computed tomography showing fluorodeoxyglucose avid lung primary