 PDF
PDF  Views
Views  Share
Share


Cerebral Sinus Venous Thrombosis in Indian Pediatric Patients With Acute Lymphoblastic Leukemia: Incidence, Risk Factors, and Outcome
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2020; 41(04): 523-529
DOI: DOI: 10.4103/ijmpo.ijmpo_206_19
Abstract
Background
Cerebral sinus venous Thrombosis (CSVT) is a rare complication of acute lymphoblastic leukemia (ALL) treatment, with an incidence rate ranging from 1.1%-to 2.9%. Steroids and L-asparaginase (LASP) are the major risk factors.
Methods
The aim of this study was to find the incidence rate and risk factors for CSVT in our patients. Ninety-two pediatric ALL diagnosed and treated with ALL-Berlin–Frankfurt–Munster-95 protocol over a period of 5 years (2013–2017) were the subject of the study. Six (6.5%) patients developed CSVT during their therapy and were further analyzed.
Results
Six (five males and one female) patients had a CSVT event. The mean age at presentation was 13.5 ± 4.1 years. CSVT event occurred during the induction/re-induction phase of chemotherapy. The superior sagittal sinus was the most frequent site of thrombosis. The timing of CSVT was related to using of LASP and steroids. High-risk disease was associated with an increased risk of thrombosis. Infection and dehydration were other important risk factors. No association was observed between the risk of CSVT and age, sex, immunophenotype, and white blood cell count. All the patients were treated with low-molecular-weight heparin and one patient developed heparin-induced thrombocytopenia. No death occurred due to CSVT.
Conclusions
The Incidence of CSVT was 6.5%-in our study which is significantly high but comparable with studies from other Asian countries. It is, therefore, important to be vigilant for the detection of CSVT during treatment of ALL and initiate the appropriate treatment to prevent adverse events.
Publication History
Received: 07 October 2019
Accepted: 10 February 2020
Article published online:
17 May 2021
© 2020. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Abstract
Background
Cerebral sinus venous Thrombosis (CSVT) is a rare complication of acute lymphoblastic leukemia (ALL) treatment, with an incidence rate ranging from 1.1%-to 2.9%. Steroids and L-asparaginase (LASP) are the major risk factors.
Methods
The aim of this study was to find the incidence rate and risk factors for CSVT in our patients. Ninety-two pediatric ALL diagnosed and treated with ALL-Berlin–Frankfurt–Munster-95 protocol over a period of 5 years (2013–2017) were the subject of the study. Six (6.5%) patients developed CSVT during their therapy and were further analyzed.
Results
Six (five males and one female) patients had a CSVT event. The mean age at presentation was 13.5 ± 4.1 years. CSVT event occurred during the induction/re-induction phase of chemotherapy. The superior sagittal sinus was the most frequent site of thrombosis. The timing of CSVT was related to using of LASP and steroids. High-risk disease was associated with an increased risk of thrombosis. Infection and dehydration were other important risk factors. No association was observed between the risk of CSVT and age, sex, immunophenotype, and white blood cell count. All the patients were treated with low-molecular-weight heparin and one patient developed heparin-induced thrombocytopenia. No death occurred due to CSVT.
Conclusions
The Incidence of CSVT was 6.5%-in our study which is significantly high but comparable with studies from other Asian countries. It is, therefore, important to be vigilant for the detection of CSVT during treatment of ALL and initiate the appropriate treatment to prevent adverse events.
Introduction
Acute lymphoblastic leukemia (ALL) is the most common childhood cancer, with an overall 5-year overall survival (OS) rate of 80%–86%-and the 5-year event-free survival (EFS) rate of approximately 78%–83%.[1] Cerebral sinus venous thrombosis (CSVT) is an important complication of ALL therapy, with a reported prevalence rate of 1.1%–2.9%.[2],[3],[4] It is associated with a mortality rate of 8%–13%-and long-term morbidity.[3] In a recent meta-analysis of several studies on venous thromboembolism (VTE) in pediatric ALL patients, the global risk of VTE has been estimated to be 5.2%, and more than 50%-of these events occurred in the central nervous system.[5] Several risk factors have been identified for the occurrence of CSVT in ALL patients such as high-risk (HR) disease, T-cell immunophenotype, drugs such as L-asparaginase (LASP) and steroids, and presence of underlying inherited thrombophilia.[2],[5],[6],[7],[8]
Almost 10,000 new cases of childhood ALL are likely diagnosed in India each year. Even with an estimated risk of 5%, over 500 new cases of thrombotic complications should be reported each year.[9] However, there is a marked paucity of data on thrombotic complications in ALL patients from India and other Asian countries, with only a few published reports.[10],[11],[12],[13] The aim of this study was to find the incidence of CSVT and identify the risk factors in our pediatric ALL patients.
Materials and Methods
Study population
In this retrospective analysis, children with ALL between 1 and 18 years of age diagnosed and treated at our institution from January 2013 to December 2017 were the subject of the study. The clinical and laboratory data were retrieved from their medical case files.
All the children who developed CSVT were further analyzed. The diagnosis and risk classification was according to the ALL-Berlin–Frankfurt–Munster (BFM)-95 protocol.[14] The patients were risk-stratified according to age, initial white blood cell (WBC) count, day 8 response to prednisolone, T-immunophenotype, and molecular re-arrangement into standard risk, medium risk (MR), and HR groups. The treatment protocol at our institute is a modification of ALL-BFM-95 protocol.[14] The induction chemotherapy consisted of four-drug phase A (daily oral prednisolone 60 mg/m2 days 1–28, once weekly intravenous vincristine 1.5 mg/m2 and daunorubicin 30 mg/m2 × 4 weeks and twice weekly intravenous LASP 5000 u/m2 × 8 doses) followed by phase B (intravenous cyclophosphamide 1000 mg/m2 on days 34 and 64, intravenous cytosine arabinoside 75 mg/m2 4 blocks of 4 days each between weeks 6 and 9, and daily oral 6-mercaptopurine (6-MP) 50 mg/m2). The consolidation/extra-compartment phase consisted of a 24-h infusion of methotrexate (MTX) 5.0 g/m2 every 2 weeks and cytosine arabinoside 200 mg/m2 for a total of 4 doses and daily oral 6-MP 25 mg/m2. The re-induction phase comprised phase A (weekly intravenous vincristine 1.5 mg/m2 and doxorubicin 30 mg/m2 × 4 weeks, LASP 10,000 μ/m2 × 4 doses during weeks 19–20, and daily oral dexamethasone 10 mg/m2) followed by phase B (single dose of intravenous cyclophosphamide 1000 mg/m2 at week 22 and two 4 days block of intravenous cytosine arabinoside 75 mg/m2 at weeks 23 and 24 and oral 6-thioguanine (6-TG) 60 mg/m2). Escherichia coli LASP was used in our patients. Central nervous system (CNS)-directed therapy consisted of intrathecal MTX (IT-MTX) 12 mg/dose administered in induction phase (2 and 3 doses in phase A and B, respectively), 4 doses in extra-compartment phase (every two weeks), and 2 doses in re-induction phase B. Patients with HR disease received 2 additional doses of IT-MTX in induction phase A and cranial radiotherapy 18 Gy in 10 fractionated doses after re-induction B phase of the chemotherapy protocol. The maintenance phase consisted of daily oral 6-MP 50 mg/m2 and weekly oral MTX 20 mg/m2. The duration of treatment in females and males was 104 and 156 weeks from the start of therapy, respectively.
Documentation of thrombotic events
The diagnosis of CSVT was done by standard radiological techniques as per the institute guidelines. Thrombosis of the cerebral vessels was diagnosed by computed tomography scan, magnetic resonance imaging (MRI) and magnetic resonance venography (MRV). Compression ultrasonography (USG) and color Doppler USG were performed to rule out deep vein thrombosis of extremities. Repeat radiological evaluation was done post 3 months of anticoagulation therapy to look for resolution of thrombosis.
Evaluation of hemostatic defects
All patients with thrombosis underwent laboratory screening for inherited thrombophilia. Laboratory evaluation included complete blood count, prothrombin time, activated partial thromboplastin time, fibrinogen level, and D-dimer assay. Prothrombotic state evaluation included measurement of antithrombin (AT) III and protein C activities by chromogenic assay and free protein S antigen levels by ELISA technique chromogenic assay. Factor V Leiden, prothrombin G20210A mutation, and MTHFR gene mutation analysis were done by molecular techniques.
Management of thrombosis
All the patients with symptomatic CSVT were treated with low-molecular-weight heparin (LMWH) (enoxaparin) 1 mg/kg every 12 hourly for the first 2 weeks and then once a day for a minimum of 3-month duration. At the end of 3 months, patients were re-evaluated radiologically for the resolution of thrombosis. If recanalization of the thrombosed vessel occurred then LMWH was stopped, if there was no or only partial recanalization of the thrombosed sinuses it was given for an additional period 3 months as per the recommended guidelines.[15] During the treatment with LMWH, patients were monitored for the occurrence of any adverse events such as bleeding and heparin-induced thrombocytopenia (HIT). Fondaparinux (indirect Factor Xa inhibitor) 0.1 mg/kg/day was used in patients who developed HIT.
Statistical analysis
Continuous variables were presented using mean ± standard deviation while categorical variables were in frequency (%). The unpaired t-test was used to compare the means while Fisher's exact test for proportions between CSVT and non-CSVT groups. Univariate binary logistic regression analysis was performed to compute odds ratio with a corresponding 95%-confidence interval. P < 0>
In this retrospective study, there are no patient-identifying data, and no new tests or interventions were performed. The study was carried out as per the institute's IRB and ethics committee's rules and guidelines, and no approval was required.
Results
Over a period of 5 years (January 2013–December 2017), 238 patients were diagnosed with ALL and were treated at our center. Ninety-two (68 males and 24 females) patients were between the ages of 1 and 18 years. The mean age was 12.01 ± 4.38 (range: 4–18) years. Seventy-four (80.4%) patients had B-cell immunophenotype and the remaining 18 (19.6%) had T-ALL. The majority of the patients had MR (76.1%) and HR (14.1%) diseases. The comparative baseline clinical and laboratory profile of pediatric ALL patients with and without CSVT is shown in [Table 1].
|
Parameter |
CSVT group (n=6) |
Non-CSVT group (n=86) |
P |
Univariate binary logistic regression analysis |
|
|---|---|---|---|---|---|
|
OR |
95% CI |
||||
|
#OR for high‑risk group was calculated after combining medium and standard risk and used as reference category. Means (unpaired t‑test) and proportions (Fisher’s exact test) were compared. Multivariate analysis was not performed as only one variable was found significant in univariate analysis. P<0> |
|||||
|
Age (years) |
|||||
|
Mean±SD (range) |
13.5±4.46 (7-18) |
11.91±4.41 (4-18) |
0.395 |
1.09 |
0.89-1.33 |
|
Age groups (years), n (%) |
|||||
|
≥10 |
4 (66.7) |
56 (65.1) |
0.997 |
1.07 0.19-6.19 |
|
|
<10> |
2 (33.3) |
30 (34.9) |
|||
|
Gender, n (%) |
|||||
|
Male |
5 (83.3) |
63 (73.3) |
0.999 |
1.83 |
0.20-16.47 |
|
Female |
1 (16.7) |
23 (26.7) |
|||
|
ALL phenotype, n (%) |
|||||
|
B-cell |
4 (66.7) |
70 (81.4) |
0.334 |
0.46 |
0.08-2.72 |
|
T-cell |
2 (33.3) |
16 (18.6) |
|||
|
Risk stratification, n (%) |
|||||
|
High risk |
4 (66.7) |
9 (10.5) |
0.006 |
17.11# |
2.74-106.93 |
|
Medium risk |
2 (33.3) |
68 (79.0) |
|||
|
Standard risk |
0 |
9 (10.5) |
|||
|
White blood cell count (at diagnosis) Mean±SD |
70.2±97.11 |
39.41±71.50 |
0.329 |
1.004 |
0.996-1.012 |
|
Median×109/L |
35.2 |
9.85 |
|||
|
CNS disease |
0 |
7 (8.1) |
- |
- |
- |
|
Prothrombotic defects |
none |
None |
- |
- |
- |
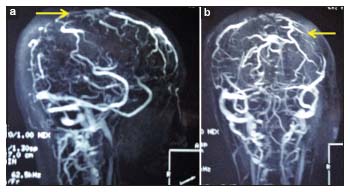
| Figure 1:(a and b) Medium‑risk venography (sagittal and coronal views) showing a partial filling defect of superior sagittal sinus suggestive of thrombosis (indicated by arrow)
The most common sites of CSVT included the sagittal sinus (5 cases), transverse sinus (4 cases), and sigmoid sinus (2 cases). Seizures (focal or generalized) were the presenting feature in all the six cases with CSVT. Headache was present in 83.3%-of cases. Neurological deficit was seen in only 1 patient (patient no. 3) who presented with left-sided hemiparesis and facial nerve palsy. This patient had extensive sinus thrombosis involving the superior sagittal sinus, bilateral transverse sinuses, straight sinuses, and cortical veins [Table 2].
|
Parameter |
Patient 1 |
Patient 2 |
Patient 3 |
Patient 4 |
Patient 5 |
Patient 6 |
|---|---|---|---|---|---|---|
|
ALL – Acute lymphoblastic leukemia; HR – High risk; MR – Medium risk; LMN – Lower motor neuron; LMWH – Low‑molecular‑weight heparin; L‑ASP – L‑asparaginase; IJV – Ïnternal juglar vein |
||||||
|
Age/sex |
17/female |
15/male |
18/male |
15/male |
9/male |
7/male |
|
ALL phenotype and risk stratification |
B-ALL HR |
B-ALL HR |
T-ALL MR |
T-ALL MR |
B-ALL HR |
B-ALL HR |
|
Chemotherapy phase |
Induction A |
Induction A |
Induction A |
Re-induction A |
Induction A |
Induction A |
|
Presenting symptoms |
Headache Altered sensorium Seizures |
Headache Seizures |
Fever Altered sensorium Neck pain and stiffness Left hemiplegia and LMN facial palsy |
Headache Seizures Todd’s paresis |
Headache Seizures |
Fever Headache Seizures |
|
Site of thrombosis |
Left transverse and sigmoid sinuses extending into left IJV |
Superior sagittal sinus, right transverse sinus |
Sagittal sinus thrombosis, bilateral transverse sinuses, straight sinuses, superficial cortical vein |
Superior sagittal sinus, bilateral transverse sinuses, left sigmoid sinus, the vein of Galen |
Superior sagittal sinus, right transverse sinus |
Superior sagittal sinus |
|
L-ASP Number of doses |
4 |
6 |
None |
2 |
6 |
None |
|
Associated risk factors |
Steroids |
Steroids |
Steroids Infection |
Steroids |
Steroids |
Steroids Infection Dehydration |
|
Anticoagulation |
LMWH |
LMWH |
LMWH |
LMWH |
LMWH |
LMWH |
|
Duration |
3 months |
2 weeks Fondaparinux 10 weeks |
6 months |
3 months |
3 months |
|
|
Long-term outcome |
No residual deficit |
No residual deficit |
Recovery of hemiparesis and facial nerve palsy |
No residual deficit |
No residual deficit |
No residual deficit |
| Figure 1:(a and b) Medium‑risk venography (sagittal and coronal views) showing a partial filling defect of superior sagittal sinus suggestive of thrombosis (indicated by arrow)
References
- Pui CH, Evans WE. Treatment of acute lymphoblastic leukemia. N Engl J Med 2006; 354: 166-78
- Qureshi A, Mitchell C, Richards S, Vora A, Goulden N. Asparaginase-related venous thrombosis in UKALL 2003- re-exposure to asparaginase is feasible and safe. Br J Haematol 2010; 149: 410-3
- Ranta S, Tuckuviene R, Makipernaa A, Albertsen BK, Frisk T, Tedgard U. et al. Cerebral venous thrombosis in children with acute lymphoblastic leukemia – A multicentric study from the Nordic society of pediatric hematology and oncology. Br J Hematol 2015; 168: 547-52
- Musgrave KM, van Delft FW, Avery P, Clack RM, Chalmers EA, Qureshi A. et al. Cerebral sinovenous thrombosis in children and young adults with acute lymphoblastic leukemia – A cohort study from the United Kingdom. Br J Hematol 2017; 179: 667-8
- Caruso V, Iacoviello L, Di Castelnuovo A, Storti S, Mariani G, de Gaetano G. et al. Thrombotic complications in childhood acute lymphoblastic leukemia: A meta-analysis of 17 prospective studies comprising 1752 pediatric patients. Blood 2006; 108: 2216-22
- Payne JH, Vora AJ. Thrombosis and acute lymphoblastic leukaemia. Br J Haematol 2007; 138: 430-45
- Nowak-Göttl U, Kenet G, Mitchell LG. Thrombosis in childhood acute lymphoblastic leukaemia: Epidemiology, aetiology, diagnosis, prevention and treatment. Best Pract Res Clin Haematol 2009; 22: 103-14
- Athale UH, Chan AK. Thrombosis in children with acute lymphoblastic leukemia: Part I. Epidemiology of thrombosis in children with acute lymphoblastic leukemia. Thromb Res 2003; 111: 125-31
- Kulkarni KP, Arora RS, Marwaha RK. Survival outcome of childhood acute lymphoblastic leukemia in India: A resource-limited perspective of more than 40 years. J Pediatr Hematol Oncol 2011; 33: 475-9
- Malhotra P, Jain S, Kapoor G. Symptomatic cerebral sinovenous thrombosis associated with L-asparaginase in children with acute lymphoblastic leukemia: A single institution experience over 17 years. J Pediatr Hematol Oncol 2018; 40: e450-3
- Lee JH, Lee J, Yhim HY, Oh D, Bang SM. Venous thromboembolism following L-asparaginase treatment for lymphoid malignancies in Korea. J Thromb Haemost 2017; 15: 655-61
- Ghanem KM, Dhayni RM, Al-Aridi C, Tarek N, Tamim H, Chan AK. et al. Cerebral sinus venous thrombosis during childhood acute lymphoblastic leukemia therapy: Risk factors and management. Pediatr Blood Cancer 2017; 64: e266-94
- Torun YA, Patiroglu T, Ozdemir MA, Ozkul Y, Ekici A, Karakukcu M. Inherited prothrombotic risk factors in Turkish children with acute lymphoblastic leukemia: Significance of concomitant genetic mutation. Clin Appl Thromb Hemost 2012; 18: 218-21
- Möricke A, Reiter A, Zimmermann M, Gadner H, Stanulla M, Dördelmann M. et al. Risk-adjusted therapy of acute lymphoblastic leukemia can decrease treatment burden and improve survival: Treatment results of 2169 unselected pediatric and adolescent patients enrolled in the trial ALL-BFM 95. Blood 2008; 111: 4477-89
- Zia AN, Chitlur M. Management of thrombotic complications in acute lymphoblastic leukemia. Indian J Pediatr 2013; 80: 853-62
- Mitchell LG, Andrew M, Hanna K, Abshire T, Halton J, Anderson R. et al. A prospective study determining the prevalence of thrombotic events in children with acute lymphoblastic leukemia and a central venous line who are treated with L-asparaguses: Results of the prophylactic anti-thrombin replacement in kids with acute lymphoblastic leukemia treated with asparaginase (PARKAA) study. Cancer 2003; 97: 508-16
- Athale UH, Siciliano SA, Crowther M, Barr RH, Chan AK. Thromboembolism in children with acute lymphoblastic leukemia treated on Dana Farber Cancer Institute protocols: Effect on age and risk stratification of disease. Br J Hematol 2005; 129: 803-10
- Sutor AH, Mall V, Thomas KB. Bleeding and thrombosis in children with acute lymphoblastic leukaemia, treated according to the ALL-BFM-90 protocol. Klin Padiatr 1999; 211: 201-4
- Mauz-Körholz C, Nürnberger W, Irsfeld H, Körholz D, Göbel U. Low rate of severe venous thromboses in children with ALL treatment according to COALL-92 and -97 protocol. Klin Padiatr 1999; 211: 215-7
- Nowak-Göttl U, Heinecke A, von Kries R, Nürnberger W, Münchow N, Junker R. Thrombotic events revisited in children with acute lymphoblastic leukemia: Impact of concomitant Escherichia coli asparaginase/prednisone administration. Thromb Res 2001; 103: 165-72
- Athale UH, Chan AK. Thrombosis in children with acute lymphoblastic leukaemia: Epidemiology of thrombosis in children with acute lymphoblastic leukaemia. Part II. Pathogenesis of thrombosis in children with acute lymphoblastic leukemia. Effects of the disease and therapy. Thrombosis Res 2003; 111: 199-212
- Hunault-Berger M, Chevallier P, Delain M, Bulabois CE, Bologna S, Bernard M. et al. Changes in antithrombin and fibrinogen levels during induction chemotherapy with L-asparaginase in adult patients with acute lymphoblastic leukemia or lymphoblastic lymphoma. Use of supportive coagulation therapy and clinical outcome: The CAPELAL study. Haematologica 2008; 93: 1488-94
- Ku GH, White RH, Chew HK, Harvey DJ, Zhou H, Wun T. Venous thromboembolism in patients with acute leukemia: Incidence, risk factors, and effect on survival. Blood 2009; 113: 3911-7
- Grace RF, Dahlberg SE, Neuberg D, Sallan SE, Connors JM, Neufeld EJ. et al. The frequency and management of asparaginase-related thrombosis in paediatric and adult patients with acute lymphoblastic leukaemia treated on Dana-Farber Cancer Institute consortium protocols. Br J Haematol 2011; 152: 452-9
- Klaassen IL, van Els AL, van de Wetering MD, van Ommen CH. Increasing incidence and recurrence rate of venous thromboembolism in paediatric oncology patients in one single centre over 25 years. Thromb Haemost 2017; 117: 2156-62
- Nowak-Göttl U, Wermes C, Junker R, Koch HG, Schobess R, Fleischhack G. et al. Prospective evaluation of the thrombotic risk in children with acute lymphoblastic leukemia carrying the MTHFR TT 677 genotype, the prothrombin G20210A variant, and further prothrombotic risk factors. Blood 1999; 93: 1595-9
- Ogawa C, Ohara A, Manabte A, Hanada R, Takashi H, Koh K. et al. Treatment outcome of discontinued L-asparaginase in children with standard-risk acute lymphoblastic leukemia: Tokyo children cancer study group (TCCSG) study L99-15 (abstract). Blood 2005; 106: 258a
- Klaassen IL, Lauw MN, Flocco M, van der Sluis IM, Pieters R, Middeldorp S. et al. Venous thromboembolism in a large cohort of children with acute lymphoblastic leukemia: Risk factors and effect on prognosis. Res Pract Thromb Haemost. Res Pract Thromb Haemost 2019; 3: 234-41
- Eden D, Hipkins R, Bradbury CA. Cerebral thrombotic complications related to l-asparaginase treatment for acute lymphoblastic leukemia: Retrospective review of 10 cases. Clin Appl Thromb Hemost 2016; 22: 589-93