 PDF
PDF  Views
Views  Share
Share


Cryptosporidiosis causing severe persistent diarrhea in a patient with multiple myeloma: A Case report and brief review of literature
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2014; 35(01): 93-95
DOI: DOI: 10.4103/0971-5851.133731
Abstract
Cryptosporidiosis is a protozoal infection that leads to self-limited diarrheal disease in immunocompetent individuals and a more severe illness in immunocompromised patients especially those infected with the human immunodeficiency virus. Although patients with hematolymphoid malignancies can develop this infection, it is an uncommon cause of diarrhea in these patients. The patient was a 64-year-old woman, a known case of multiple myeloma for 17 years, who had been treated with multiple lines of chemotherapy earlier. She was being treated with lenalidomide plus dexamethasone for active myeloma at the time of this episode. She presented with profuse watery diarrhea of 15 days duration that was proven to be due to Cryptosporidium parvum on stool examination. The diarrheal illness resolved after treatment with nitazoxanide. Although uncommon, cryptosporidial infection should be suspected in patients with hematological malignancies who have persistent diarrhea. Stool examination with the modified acid-fast Kenyoun stain establishes the diagnosis in the majority of cases. Antiparasitic treatment is effective in controlling the infection.
Publication History
Article published online:
19 July 2021
© 2014. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Abstract
Cryptosporidiosis is a protozoal infection that leads to self-limited diarrheal disease in immunocompetent individuals and a more severe illness in immunocompromised patients especially those infected with the human immunodeficiency virus. Although patients with hematolymphoid malignancies can develop this infection, it is an uncommon cause of diarrhea in these patients. The patient was a 64-year-old woman, a known case of multiple myeloma for 17 years, who had been treated with multiple lines of chemotherapy earlier. She was being treated with lenalidomide plus dexamethasone for active myeloma at the time of this episode. She presented with profuse watery diarrhea of 15 days duration that was proven to be due to Cryptosporidium parvum on stool examination. The diarrheal illness resolved after treatment with nitazoxanide. Although uncommon, cryptosporidial infection should be suspected in patients with hematological malignancies who have persistent diarrhea. Stool examination with the modified acid-fast Kenyoun stain establishes the diagnosis in the majority of cases. Antiparasitic treatment is effective in controlling the infection.
INTRODUCTION
Cryptosporidiosis is a parasitic disease that causes diarrhea lasting for about 1-2 weeks among the immunocompetent and becoming a more severe life-threatening illness among immunocompromised individuals. It constitutes 24% of human immunodeficiency virus (HIV) positive patients with diarrhea compared with 6.1% in the immunocompetent individuals. Association of cryptosporidiosis with malignancies is not as robust as acquired immunodeficiency syndrome (AIDS). Here, we report a case of cryptosporidiosis causing severe persistent diarrhea in a patient with multiple myeloma.
CASE REPORT
The case we present here is the patient was a 64-year-old female who had been diagnosed to have multiple myeloma, stage III B, type IgG kappa 17 years ago in 1993. She had received multiple lines of chemotherapy during this period. There was no history of other comorbidities such as diabetes, hypertension or tuberculosis. She was being treated with oral lenalidomide (25 mg for 21 days) and dexamethasone (40 mg on days 1, 8 and 15) of 28 days cycle for the current progression of myeloma. The baseline serum M band prior to the start of this regimen was 3.4 g/dl.
She presented on day 17 of the 2nd cycle with the complaints of profuse watery diarrhea, 10-12 times/day for the previous 15 days. The diarrheal product was non-bloody, without any mucus and not foul smelling. This was associated with nausea, mild crampy abdominal pain and a sense of fecal urgency without any fever. Physical examination was unremarkable except for tachycardia and signs of mild dehydration. There was anemia (hemoglobin of 9.7 g/dl) and leucopenia (white blood cells count 2800/mm3) but the absolute neutrophil count (1700/mm3) and platelets were normal. The liver and renal function tests were within normal limits but serum potassium was low (2.2 meq/L). Serological tests for HIV and hepatitis B and C were negative. The routine blood culture was sterile and the polymerase chain reaction test in peripheral blood for cytomegalovirus deoxyribonucleic acid was negative.
Stool examination showed 2-3 polymorphonuclear leucocytes per high power field with mucus but no visible or occult blood. No pathogen was seen on the gram stain and grown in culture. She was started on injectable cefoperazone-sulbactam and netilmicin but the diarrhea continued. Colonoscopy was performed, which suggested colonic mucosal inflammation likely to be infective in origin [Figure 1]. At this point, a diagnosis of cryptosporidial infection was suspected and the stool was submitted for examination with the modified Kinyoun acid-fast stain. This revealed multiple oocysts of Cryptosporidium parvum [Figure 2]. The patient was then started on oral nitazoxanide 500 mg 12 hourly for 10 days. The diarrheal frequency decreased after 5 days and it resolved completely by the 10th day of this drug. The patient was able to resume treatment with lenalidomide and dexamethasone later without any complications.
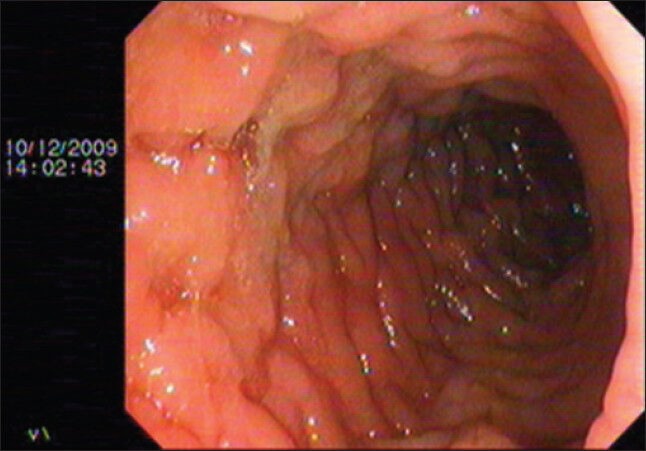
| Figure 1:Colonic mucosal inflammation on colonoscopy of the patient
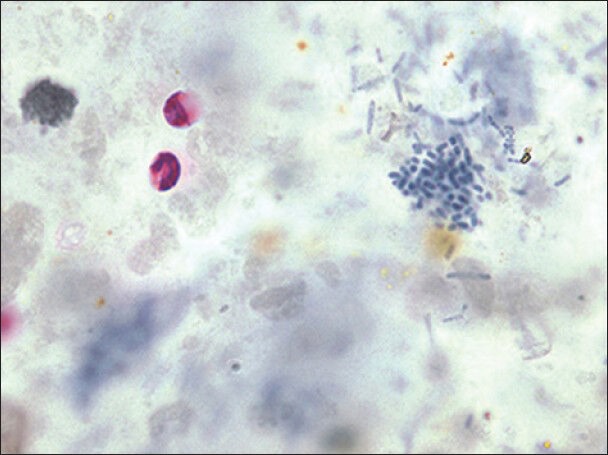
| Figure 2:Oocysts of Cryptosporidium parvum in modified Kinyoun acid-fast stain
DISCUSSION
Cryptosporidiosis is a protozoal intestinal infection caused by many species of the genus Cryptosporidium that are either obligate human or human and bovine parasites. The first association with human diarrheal disease was reported in 1976, one case in an otherwise healthy child and one in an immunosuppressed adult.[1,2] The infection is acquired by ingesting parasites in water or food contaminated by human or animal feces or by having contact with soil, a person, or an item that has been contaminated with the parasite. The diagnosis is established by demonstration of oocysts in the stool by the modified acid-fast Kinyoun stain.[3]
Since the initial reports, its strongest association has been with patients of AIDS caused by HIV. Four clinical syndromes of cryptosporidial infection have been described in HIV positive patients: Chronic diarrhea (affecting 36% of patients), cholera-like disease (33%), transient diarrhea (15%) and relapsing illness (15%).[4] The severity of illness is related to the CD4 count in these patients. In immunocompetent patients, usually children <5>
Although uncommon, cryptosporidial diarrhea has been described in patients with malignancy. In one study, the incidence of cryptosporidiosis was 1.3% in the 560 cancer patients presenting with symptoms of diarrhea out of which 71% had hematolymphoid malignancy.[5] In other studies it was found that the risk of severe disease is largely limited to children with acute leukemia and lymphoma.[6,7,8,9] Interestingly, bone marrow transplantation does not seem to confer any additional risk over that of the underlying disease.[8]
CONCLUSION
Cryptosporidial diarrhea should be included in the differential diagnosis of any patient with persistent severe diarrhea, especially in patients with hematological malignancies. Diagnosis can be established by stool examination and administration of nitazoxanide is effective in controlling the infection.[10]
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- Crawford FG, Vermund SH. Human cryptosporidiosis. Crit Rev Microbiol 1988;16:113-59.
- Meisel JL, Perera DR, Meligro C, Rubin CE. Overwhelming watery diarrhea associated with a Cryptosporidium in an immunosuppressed patient. Gastroenterology 1976;70:1156-60.
- Magi B, Canocchi V, Tordini G, Cellesi C, Barberi A. Cryptosporidium infection: Diagnostic techniques. Parasitol Res 2006;98:150-2.
- Manabe YC, Clark DP, Moore RD, Lumadue JA, Dahlman HR, Belitsos PC, et al. Cryptosporidiosis in patients with AIDS: Correlates of disease and survival. Clin Infect Dis 1998;27:536-42.
- Sreedharan A, Jayshree RS, Sridhar H. Cryptosporidiosis among cancer patients: An observation. J Diarrhoeal Dis Res 1996;14:211-3.
- Foot AB, Oakhill A, Mott MG. Cryptosporidiosis and acute leukaemia. Arch Dis Child 1990;65:236-7.
- Gentile G, Caprioli A, Donelli G, Venditti M, Mandelli F, Martino P. Asymptomatic carriage of Cryptosporidium in two patients with leukemia. Am J Infect Control 1990;18:127-8.
- Gentile G, Venditti M, Micozzi A, Caprioli A, Donelli G, Tirindelli C, et al. Cryptosporidiosis in patients with hematologic malignancies. Rev Infect Dis 1991;13:842-6.
- Travis WD, Schmidt K, MacLowry JD, Masur H, Condron KS, Fojo AT. Respiratory cryptosporidiosis in a patient with malignant lymphoma. Report of a case and review of the literature. Arch Pathol Lab Med 1990;114:519-22.
- Rossignol JF, Ayoub A, Ayers MS. Treatment of diarrhea caused by Cryptosporidium parvum: A prospective randomized, double-blind, placebo-controlled study of Nitazoxanide. J Infect Dis 2001;184:103-6.
| Figure 1:Colonic mucosal inflammation on colonoscopy of the patient
| Figure 2:Oocysts of Cryptosporidium parvum in modified Kinyoun acid-fast stain
References
- Crawford FG, Vermund SH. Human cryptosporidiosis. Crit Rev Microbiol 1988;16:113-59.
- Meisel JL, Perera DR, Meligro C, Rubin CE. Overwhelming watery diarrhea associated with a Cryptosporidium in an immunosuppressed patient. Gastroenterology 1976;70:1156-60.
- Magi B, Canocchi V, Tordini G, Cellesi C, Barberi A. Cryptosporidium infection: Diagnostic techniques. Parasitol Res 2006;98:150-2.
- Manabe YC, Clark DP, Moore RD, Lumadue JA, Dahlman HR, Belitsos PC, et al. Cryptosporidiosis in patients with AIDS: Correlates of disease and survival. Clin Infect Dis 1998;27:536-42.
- Sreedharan A, Jayshree RS, Sridhar H. Cryptosporidiosis among cancer patients: An observation. J Diarrhoeal Dis Res 1996;14:211-3.
- Foot AB, Oakhill A, Mott MG. Cryptosporidiosis and acute leukaemia. Arch Dis Child 1990;65:236-7.
- Gentile G, Caprioli A, Donelli G, Venditti M, Mandelli F, Martino P. Asymptomatic carriage of Cryptosporidium in two patients with leukemia. Am J Infect Control 1990;18:127-8.
- Gentile G, Venditti M, Micozzi A, Caprioli A, Donelli G, Tirindelli C, et al. Cryptosporidiosis in patients with hematologic malignancies. Rev Infect Dis 1991;13:842-6.
- Travis WD, Schmidt K, MacLowry JD, Masur H, Condron KS, Fojo AT. Respiratory cryptosporidiosis in a patient with malignant lymphoma. Report of a case and review of the literature. Arch Pathol Lab Med 1990;114:519-22.
- Rossignol JF, Ayoub A, Ayers MS. Treatment of diarrhea caused by Cryptosporidium parvum: A prospective randomized, double-blind, placebo-controlled study of Nitazoxanide. J Infect Dis 2001;184:103-6.