 PDF
PDF  Views
Views  Share
Share


Cytomegalovirus Retinitis Occurring as a Complication of HyperCVAD Chemotherapy: Report of Two Cases
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2018; 39(04): 548-550
DOI: DOI: 10.4103/ijmpo.ijmpo_48_17
Abstract
Cytomegalovirus (CMV) retinitis is usually diagnosed in patients with acquired immunodeficiency syndrome and in solid organ and hematopoietic stem cell transplant recipients. It produces a characteristic necrotizing retinitis which is a sight-threatening condition in these patients. CMV retinitis occurs rarely in patients undergoing only chemotherapy, and very few cases have been reported during the maintenance phase of acute lymphoblastic leukemia (ALL) in children. We report two patients, one with ALL and the other with Burkitt’s lymphoma on HyperCVAD chemotherapy developing CMV retinitis during the course of treatment. Both patients were treated with intravenous ganciclovir, oral valganciclovir and intravitreal ganciclovir. Both patients are alive in remission at 60 and 40 months, respectively, with preservation of normal vision.
Publication History
Article published online:
17 June 2021
© 2018. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Abstract
Cytomegalovirus (CMV) retinitis is usually diagnosed in patients with acquired immunodeficiency syndrome and in solid organ and hematopoietic stem cell transplant recipients. It produces a characteristic necrotizing retinitis which is a sight-threatening condition in these patients. CMV retinitis occurs rarely in patients undergoing only chemotherapy, and very few cases have been reported during the maintenance phase of acute lymphoblastic leukemia (ALL) in children. We report two patients, one with ALL and the other with Burkitt’s lymphoma on HyperCVAD chemotherapy developing CMV retinitis during the course of treatment. Both patients were treated with intravenous ganciclovir, oral valganciclovir and intravitreal ganciclovir. Both patients are alive in remission at 60 and 40 months, respectively, with preservation of normal vision.
Introduction
Primary cytomegalovirus (CMV) infection is usually asymptomatic in immunocompetent individuals; however, in immunosuppressed hosts, the infection causes retinitis, gastroenteritis, colitis, pneumonitis, and encephalitis and results in significant morbidity and mortality. CMV produces a characteristic necrotizing retinitis which is a sight-threatening condition. It occurs rarely in patients undergoing only chemotherapy. Few cases have been reported during the maintenance phase of acute lymphoblastic leukemia (ALL) in children.[1] We report 2 patients on HyperCVAD chemotherapy developing CMV retinitis while on treatment.
Case Reports
Patient 1
A 16-year-old boy was diagnosed with T-cell ALL and was started on HyperCVAD regimen. He attained marrow remission after cycle IA and was continued till IV B, followed by prophylactic cranial radiation and maintenance chemotherapy with oral 6-mercaptopurine and methotrexate. One year later, he presented with decreased vision in the left eye. Ophthalmologic examination showed granular variant of CMV retinitis [Figure 1]. His absolute CD4 count was 134 cells/μL and serum CMV quantitative polymerase chain reaction (QPCR) was 63 IU/ml. He was started on intravenous ganciclovir 6 mg/kg/day for 21 days followed by oral valganciclovir 900 mg twice daily for another 3 weeks. He also received intravitreal ganciclovir injection, 2.25 mg at week 4. His CMV QPCR became undetectable 2 weeks after starting therapy. The patient regained normal vision, and an ophthalmology review after 5 weeks of therapy showed healed CMV retinitis. His absolute CD4 count improved, and he completed 2 years of maintenance chemotherapy. Ophthalmic examination after completion of treatment showed fresh CMV retinitis lesions in the right eye and healed lesions in the left eye. He was restarted on weekly intravitreal ganciclovir injection 2.25 mg for 2 doses along with oral valganciclovir for 2 months following which his ocular lesions healed and he also underwent laser barrage of healed left eye. Currently, he continues to be in complete remission of his leukemia and his CMV retinitis at 60 months.
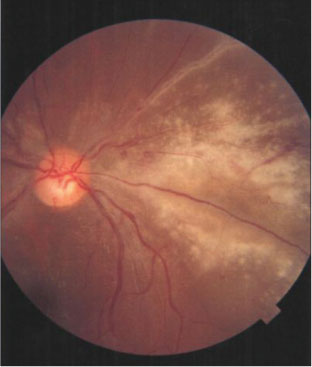
| Figure 1:Retina of the left eye of patient 1 showing active granular cytomegalovirus retinitis
Patient 2
A 32-year-old man was diagnosed with Burkitt’s lymphoma and started on HyperCVAD chemotherapy along with Rituximab (R HyperCVAD). Following the cycle 4 A, he complained of defective vision in the left eye. The ophthalmologic examination revealed bilateral acute retinitis; left more than right [Figure 2]. His CMV IgG was positive, serum CMV QPCR was 1,20,150 IU/ml, and absolute CD4 count was 45 cells/μL. He was given intravenous ganciclovir 6 mg/kg/day for 21 days followed by oral valganciclovir. The CMV QPCR titers became normal after 3 weeks of therapy. He also had profound myelosuppression during this period. A repeat ophthalmologic evaluation showed good resolution of retinitis and vision was preserved. The CMV QPCR became undetectable after 9 weeks, valganciclovir was discontinued after 15 weeks, and he was kept on follow-up. After 3 months, the ophthalmologic evaluation showed few hemorrhagic lesions in the right eye and oral valganciclovir was restarted at 900 mg once daily. He responded, ocular lesions healed, and the drug was stopped after 12 weeks. At present, he is in complete remission at 40 months. His CMV retinitis also has completely resolved with preservation of normal vision.

| Figure.2:Retina of the left eye of patient 2 showing active cytomegalovirus retinitis
Discussion
The incidence of CMV antigenemia in adults with lymphoid malignancies who did not undergo stem cell transplant was reported as 13.6%.[2] The rate of CMV reactivation in patients with hematologic malignancies in the nontransplant setting was highest for alemtuzumab therapy (50%), followed by 9.7% for HyperCVAD regimen and 4.6% for fludarabine-based regimes.[3] The incidence of CMV retinitis affecting children with ALL in the nontransplant setting was estimated as 3.6%, but no data is available in adults.[4] CMV retinitis presents as a necrotizing retinitis with a characteristic ophthalmoscopic appearance, is usually unilateral, but may progress to opposite eye if inadequately treated and may result in visual loss.
Both the patients in this report were on HyperCVAD chemotherapy when they developed the CMV retinitis. There are only 3 other reports in world literature on patients developing CMV retinitis while on HyperCVAD. A 39-year-old female with Burkitt’s lymphoma on RHyperCVAD developed CMV retinitis and was treated with intravenous ganciclovir, intravitreal ganciclovir, and intravenous foscarnet.[5] Another 50-year-old man with T-cell ALL developed CMV retinitis during 4th cycle of R HyperCVAD and was treated with oral valganciclovir.[6] A 49-year-old man with ALL, on salvage chemotherapy with HyperCVAD, developed CMV retinitis and was treated with intravenous ganciclovir with preservation of visual acuity.[7]
There is profound immunosuppression during the maintenance phase of ALL. The reconstitution of B-cell and natural killer cells occur early, whereas the T-helper and T-suppressor cell recovery are delayed.[8] In addition, there is low absolute lymphocyte count, low CD4 T-cells, and immunoglobulins. The addition of vincristine and dexamethasone pulses to 6-mercaptoputine and methotrexate may affect cell-mediated immunity and increase the risk of CMV retinitis.[9]
In both patients in this report, CMV retinitis was diagnosed clinically along with elevated plasma CMV DNA and reduced CD4 counts. Intraocular fluid sampling was not done in view of the thrombocytopenia. Both responded to initial ganciclovir, however, had asymptomatic relapse and were successfully treated with a second course of ganciclovir. Currently, both patients are in complete remission of their primary disease as well as the CMV status and have normal vision. The possible factors that predisposed our patients to develop CMV retinitis could be the immunosuppression inherent to the disease and to the intensive chemotherapy in addition to the high dose of steroids in HyperCVAD.
Early and prompt treatment for CMV retinitis is critical. Optimal treatment of CMV retinitis includes intravenous ganciclovir, oral valganciclovir, intravitreal ganciclovir, intravenous foscarnet, and cidofovir. Induction is usually given for 2–3 weeks followed by maintenance. Although these antivirals provide effective treatment options, phenotypic resistance to these has been reported in 5%–25%.[10] An ophthalmologist should also be included in the active management of CMV retinitis. Indirect ophthalmoscopy should be performed at the time of diagnosis, 2 weeks after initiating therapy, and monthly thereafter while patient on anti-CMV treatment to evaluate efficacy of treatment and to detect complications such as retinal detachment.
Conflict of Interest
There are no conflicts of interest.
References
- Rahbarimanesh A, Ehsani M, Karahroudi M, Rashidi A, Aghajani M, Meysami A. et al. Cytomegalovirus disease in children with acute lymphoblastic leukemia in the nontransplant setting: Case series and review of the literature. J Pediatr Hematol Oncol 2015; 37: 429-32
- Han XY. Epidemiologic analysis of reactivated cytomegalovirus antigenemia in patients with cancer. J Clin Microbiol 2007; 45: 1126-32
- Ng AP, Worth L, Chen L, Seymour JF, Prince HM, Slavin M. et al. Cytomegalovirus DNAemia and disease: Incidence, natural history and management in settings other than allogeneic stem cell transplantation. Haematologica 2005; 90: 1672-9
- Samia L, Hamam R, Dbaibo G, Saab R, El-Solh H, Abboud M. et al. Cytomegalovirus retinitis in children and young adults with acute lymphoblastic leukemia in Lebanon. Leuk Lymphoma 2014; 55: 1918-21
- Moss HB, Chavala S, Say E, Miller MB. Ganciclovir-resistant cytomegalovirus (CMV) retinitis in a patient with wild-type CMV in her plasma. J Clin Microbiol 2012; 50: 1796-9
- Libby E, Movva S, Quintana D, Abdul-Jaleel M, Das A. Cytomegalovirus retinitis during chemotherapy with rituximab plus hyperfractionated cyclophosphamide, vincristine, doxorubicin, and dexamethasone. J Clin Oncol 2010; 28: e661-2
- Taha R, Al Hijji I, El Omri H, Al-Laftah F, Negm R, Yassin M. et al. two ocular infections during conventional chemotherapy in a patient with acute lymphoblastic leukemia: A case report. Case Rep Oncol 2010; 3: 234-239
- El-Chennawi FA, Al-Tonbary YA, Mossad YM, Ahmed MA. Immune reconstitution during maintenance therapy in children with acute lymphoblastic leukemia, relation to co-existing infection. Hematology 2008; 13: 203-9
- Moritake H, Kamimura S, Kojima H, Shimonodan H, Harada M, Sugimoto T. et al. Cytomegalovirus retinitis as an adverse immunological effect of pulses of vincristine and dexamethasone in maintenance therapy for childhood acute lymphoblastic leukemia. Pediatr Blood Cancer 2013; 60: 329-31
- Chou S. Phenotypic diversity of cytomegalovirus DNA polymerase gene variants observed after antiviral therapy. J Clin Virol 2011; 50: 287-91
Address for correspondence
Publication History
Article published online:
17 June 2021
© 2018. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2,
Noida-201301 UP, India
| Figure 1:Retina of the left eye of patient 1 showing active granular cytomegalovirus retinitis
| Figure.2:Retina of the left eye of patient 2 showing active cytomegalovirus retinitis
References
- Rahbarimanesh A, Ehsani M, Karahroudi M, Rashidi A, Aghajani M, Meysami A. et al. Cytomegalovirus disease in children with acute lymphoblastic leukemia in the nontransplant setting: Case series and review of the literature. J Pediatr Hematol Oncol 2015; 37: 429-32
- Han XY. Epidemiologic analysis of reactivated cytomegalovirus antigenemia in patients with cancer. J Clin Microbiol 2007; 45: 1126-32
- Ng AP, Worth L, Chen L, Seymour JF, Prince HM, Slavin M. et al. Cytomegalovirus DNAemia and disease: Incidence, natural history and management in settings other than allogeneic stem cell transplantation. Haematologica 2005; 90: 1672-9
- Samia L, Hamam R, Dbaibo G, Saab R, El-Solh H, Abboud M. et al. Cytomegalovirus retinitis in children and young adults with acute lymphoblastic leukemia in Lebanon. Leuk Lymphoma 2014; 55: 1918-21
- Moss HB, Chavala S, Say E, Miller MB. Ganciclovir-resistant cytomegalovirus (CMV) retinitis in a patient with wild-type CMV in her plasma. J Clin Microbiol 2012; 50: 1796-9
- Libby E, Movva S, Quintana D, Abdul-Jaleel M, Das A. Cytomegalovirus retinitis during chemotherapy with rituximab plus hyperfractionated cyclophosphamide, vincristine, doxorubicin, and dexamethasone. J Clin Oncol 2010; 28: e661-2
- Taha R, Al Hijji I, El Omri H, Al-Laftah F, Negm R, Yassin M. et al. two ocular infections during conventional chemotherapy in a patient with acute lymphoblastic leukemia: A case report. Case Rep Oncol 2010; 3: 234-239
- El-Chennawi FA, Al-Tonbary YA, Mossad YM, Ahmed MA. Immune reconstitution during maintenance therapy in children with acute lymphoblastic leukemia, relation to co-existing infection. Hematology 2008; 13: 203-9
- Moritake H, Kamimura S, Kojima H, Shimonodan H, Harada M, Sugimoto T. et al. Cytomegalovirus retinitis as an adverse immunological effect of pulses of vincristine and dexamethasone in maintenance therapy for childhood acute lymphoblastic leukemia. Pediatr Blood Cancer 2013; 60: 329-31
- Chou S. Phenotypic diversity of cytomegalovirus DNA polymerase gene variants observed after antiviral therapy. J Clin Virol 2011; 50: 287-91