 PDF
PDF  Views
Views  Share
Share


Hairy Cell Leukemia: Morphological and Immunophenotypic Characteristics of Seven Cases and Cyclin D1 Expression
CC BY-NC-ND 4.0 ? Indian J Med Paediatr Oncol 2021; 42(06): 595-598
DOI: DOI: 10.1055/s-0041-1736431
Abstract
Aberrant immunophenotypic expression in hairy cell leukemia (HCL), both at medullary and extramedullary sites, is not uncommonly reported in literature. Cyclin D1 positivity in HCL may mimic mantle cell lymphoma (MCL) morphologically, especially in the presence of aberrant CD5 immunopositivity, requiring?BRAFV600E?mutation and/or?CCND1?gene testing for confirmation. Here, we describe seven cases of HCL with clinicomorphological and immunophenotypic characteristics with an emphasis on cyclin D1 expression using immunohistochemistry (IHC) with a brief comprehensive literature review. We suggest that cyclin D1 positive HCL may be a distinct subtype which requires further immunophenotypic and molecular characterization for accurate diagnosis and planning of definitive therapy.
Keywords
hairy cell leukemia - trephine biopsy - translocation - therapyAuthors' Contributions
S.N.: data collection and analysis, literature review, writing of the first manuscript draft. S.P.: conceptual design, diagnosis, data analysis, literature review, review, and editing of manuscript. A.K.A. and S.P.: interpretation of data, diagnosis, and review of manuscript for intellectual contents. A.P. and P.K.D.: management of cases and review of manuscript for intellectual content.
Supplementary MaterialPublication History
30 December 2021 (online)
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Abstract
Aberrant immunophenotypic expression in hairy cell leukemia (HCL), both at medullary and extramedullary sites, is not uncommonly reported in literature. Cyclin D1 positivity in HCL may mimic mantle cell lymphoma (MCL) morphologically, especially in the presence of aberrant CD5 immunopositivity, requiring?BRAFV600E?mutation and/or?CCND1?gene testing for confirmation. Here, we describe seven cases of HCL with clinicomorphological and immunophenotypic characteristics with an emphasis on cyclin D1 expression using immunohistochemistry (IHC) with a brief comprehensive literature review. We suggest that cyclin D1 positive HCL may be a distinct subtype which requires further immunophenotypic and molecular characterization for accurate diagnosis and planning of definitive therapy.
Keywords
hairy cell leukemia - trephine biopsy - translocation - therapy
Introduction
Hairy cell leukemia (HCL) is a relatively rare, mature B-cell neoplasm, characterized by the proliferation of small mature lymphoid cells with characteristic circumferential hair-like cytoplasmic projections (hairy cells) in peripheral blood (PB) and/or in bone marrow (BM) aspirate smear, and a distinct perinuclear halo, giving a fried egg appearance in BM trephine biopsy (BMBx) sections producing reticulin fibrosis, cytopenia(s), and splenomegaly.[1] Activating mutations in the?BRAF?kinase domain at?V600E?is the hallmark molecular abnormality that promotes cell survival.[2] While flow cytometric or immunohistochemical expression of CD11c, CD103, CD123, CD25 by the lesion cells is characteristic for diagnosis, atypical clinical presentation involving rare extramedullary anatomic sites is not uncommon; and aberrant immunophenotypic expression of antigens such as CD5, CD23, CD10, and cyclin D1 may create a diagnostic dilemma leading to misdiagnosis.[3] [4] In this manuscript, we describe seven cases of HCL, describing their BM morphology and immunophenotypic characteristics with a focus on aberrant cyclin D1 expression in such a neoplasm with a brief literature review.
Case Presentation
We retrospectively (April 2016?August 2020) reviewed the records and slides of all the cases reported to have BM involvement in lymphoproliferative neoplasm (LPN) with a ?fried egg? or ?fried egg like? appearance on trephine biopsy. The trephine core was fixed in 10% neutral buffered formalin followed by decalcification using 14?TA (ethylene diamine tetraacetic acid) before paraffin embedding. The 4-?m deparaffinized sections were subjected to hematoxylin and eosin and reticulin staining for routine morphological analysis as per protocol. The ?fried egg? or ?fried egg like? areas were described semiquantitatively as <25>50% of the total evaluated marrow surface area. Following that, a panel of antibodies was used for characterization of lymphoid infiltrates by immunohistochemistry (IHC) on BMBx: CD3 (1:100), CD20 (1:100), CD5 (prediluted), CD23 (prediluted), CD10 (prediluted), PAX5 (prediluted), BCL2 (1:100), BCL6 (prediluted), cyclin D1 (prediluted), and Mib 1 (1:150). Annexin A1 antibody (polyclonal, Invitrogen, 1:6500) was used to confirm or rule out the HCL diagnosis in all these cases. Flow cytometry immunophenotyping data were reviewed wherever available.
HCL constituted seven of the total eleven cases of LPN (six; classical HCL one; variant HCL [vHCL]; [Supplementary Table S1] [available in the online version]). Classical HCL cases exhibited the following features:
-
Median age at diagnosis; 56 years (range: 40?70 years).
-
Splenomegaly in all except one (case no.4).
-
Peripheral blood cytopenia with lymphocyte predominance and the presence of hairy cells in all.
-
Diffuse marrow infiltrate in all except one (vHCL).
-
MF grades 2 to 3 reticulin fibrosis.
-
Strong diffuse nuclear and cytoplasmic positivity for annexin A1 in five of six cases (where performed).
Besides this, IHC revealed weak to intermediate intensity of nuclear positivity for cyclin D1 (in >30% of cell nuclei; SOX11 negative) in two cases (case nos. 5 and 7), whereas weak CD5, CD10, and CD23 positivity was noted in three cases. Both the cyclin D1 positive HCL cases lacked CD5 expression as detected by flow cytometry and IHC ([Figs. 1] and [2]; [Supplementary Fig. S1] [available in the online version]). Molecular testing by reverse transcriptase polymerase chain reaction (RT-PCR; performed on paraffin block) confirmed the presence of?BRAFV600E?mutation (c.1799T?>?A) in both the cases with cyclin D1 positivity; and translocation t(11;14) (q13; q32) was not performed in any of the cases.
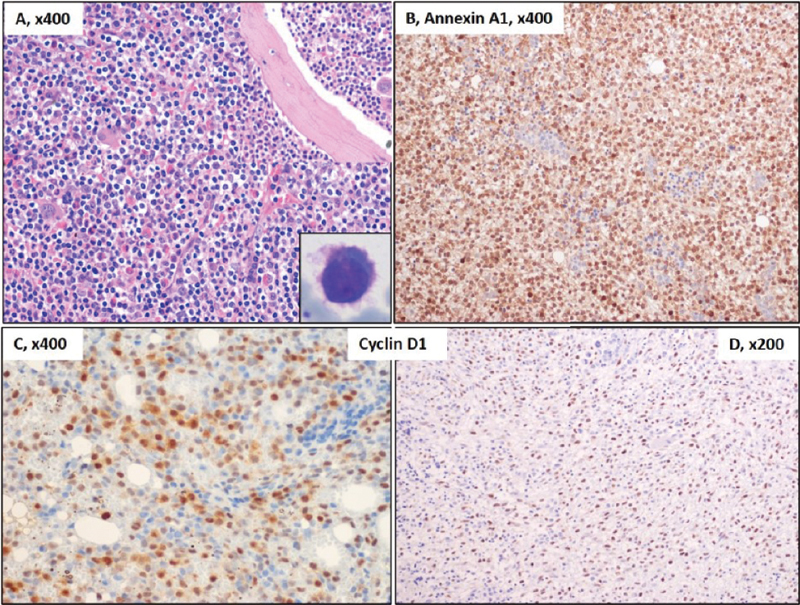
|?Fig. 1Bone marrow trephine biopsy in hairy cell leukemia showing diffuse infiltrate of lymphoid cells with a perinuclear halo giving a ?fried egg? appearance (A). Hematoxylin and eosin staining. Characteristic lymphoid cells with circumferential fine hair like projection (inset, right lower) seen in peripheral blood (Leishman?Giemsa stain, ?400) (B). Diffuse infiltrating lymphoid cells displaying strong positive results for Annexin A1 antibody test. Cyclin D1 nuclear positivity in two of the cases (C) weak to intermediate, case no. 5 (D) strong, case no. 7 ([Supplementary Table S1]). The remainder of the cases were negative for cyclin D1 (peroxidase?antiperoxidase).
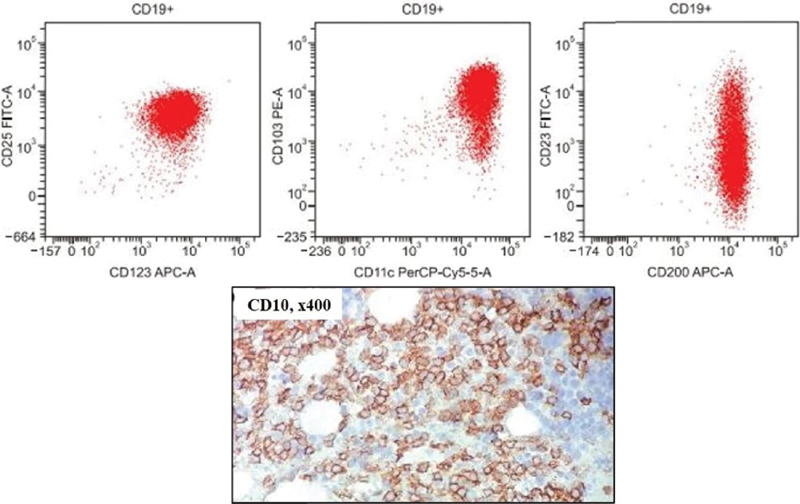
|?Fig. 2Flow cytometric immunophenotyping plots (in one of our cases) with the population of interest (B-cells) gated in red on CD19 versus side-scattered light (SSC). The neoplastic B-cells were positive for CD11c (bright), CD25 (bright), CD200, CD103, and CD123, thus diagnostic of hairy cell leukemia. Note the dim to moderate CD23 positivity in the CD19+ lymphoid cells as previously reported in the literature. These cells also express aberrant CD10 positivity on IHC (reproduced with permission from Pattnaik et al[3]).
Discussion
Aberrant immunophenotypic expression is not uncommonly reported in cases with HCL.[3] [4] A literature review on 27 cases of CD5-positive HCL by Jain et al have reported such aberrancies to occur more frequently in variant than classical HCLs (8.8 vs. 2.3%, respectively) which may be associated with aberrant CD23 positivity and unmutated?BRAFV600E?in a subset of cases.[4] Cyclin D1, encoded by?CCND1?gene, is a cell cycle regulator that promotes the G1-S phase transition. Amplification or overexpression of?CCND1?gene, secondary to translocation t(11;14) (q13; q32), is a characteristic molecular event seen in mantle cell lymphoma (MCL).[5] Cyclin D1 expression in HCL has been sporadically reported in literature with diverse clinical implications.[5] [6] [7] [8] [9] [10] [11] [12] Cortazar et al reported immunoexpression of cyclin D1 (weak?strong), CD43, CD10, and CD5 in 70, 55, 38, and 10% of their 13 cases, respectively, at extramedullary sites. All, except two, had prior or concurrent evidence of BM involvement. They suggested that CD43 and CD10 expression in HCL may be more common in extramedullary sites; both SOX11 expression and testing for t(11;14) (q13; q32) are necessary for accurate diagnosis.[5]
Rahman et al described a new variant of HCL, harboring both the mutated?BRAFV600E?gene (by PCR) and t(11;14) (q13; q32)?CCND1/IGH?fusion (by FISH [fluorescence in situ hybridization]) in an elderly male with pancytopenia displaying an excellent response to intravenous cladribine.[6] Using IHC on BM trephine biopsies, Miranda et al reported a weak cyclin D1 expression in a subpopulation of tumor cells in all cases of HCL in contrast to a stronger nuclear positivity in MCL (n?=?13).[8] Sherman et al reported a weak-intermediate nuclear positivity for cyclin D1 in a very high proportion (97/101, 96%) of HCL cases; and this along with annexin A1 positivity had higher sensitivity and specificity in ruling out other low-grade LPNs like splenic MZL and extra nodal MZL.[9] Chen et al described an unusual case of HCL which resembled a histologically nonnodal indolent variant of MCL with CD5 and cyclin D1 coexpression leading to misdiagnosis and a poor initial therapeutic response to MCL directive therapy and the subsequent relapse after years of follow-up. Molecular analysis (on relapse) demonstrated?IGVH3?74?somatic hypermutation and?CCND1-IGH?fusion by FISH, a finding very uncommonly reported in MCL, but rather commonly in HCL, leading to a favorable clinical outcome following cladribine therapy.[10] Another report described an unusual case of CD5negative, CD23negative, and CD10positive?low-grade B-cell LPN of HCL phenotype presenting as a skull base lesion, cranial nerve palsy, and displaying marrow involvement (CD11cpositive, CD25positive, and CD103positive?by flow cytometry) with diffuse and strong cyclin D1 positivity at both sites without t(11;14) abnormality. However, a good response to rituximab and cladribine-based therapy was observed.[11] Translocation t(11;20) was implicated in cyclin D1 overexpression in HCL in a Japanese patient, where the molecular expression of the same was demonstrated by Northern blot and RT-PCR studies.[12]
In summary, aberrant immunophenotypic expression of CD5, CD23, CD10, and cyclin D1 by HCL is not uncommon which needs to be kept in mind while evaluating cases of low-grade lymphoproliferative neoplasm, both at medullary and extramedullary sites. SOX11 immunophenotyping and/or molecular testing for?BRAFV600E?mutation and?CCND1?gene analysis may be required in such cases before initiating definitive therapy.
Conflict of Interest
None declared.
Authors' Contributions
S.N.: data collection and analysis, literature review, writing of the first manuscript draft. S.P.: conceptual design, diagnosis, data analysis, literature review, review, and editing of manuscript. A.K.A. and S.P.: interpretation of data, diagnosis, and review of manuscript for intellectual contents. A.P. and P.K.D.: management of cases and review of manuscript for intellectual content.
Supplementary MaterialReferences
- ?th-Lipt?k J, Piukovics K, Borb?nyi Z, Demeter J, Bagdi E, Kren?cs L.?A comprehensive immunophenotypic marker analysis of hairy cell leukemia in paraffin-embedded bone marrow trephine biopsies?a tissue microarray study. Pathol Oncol Res 2015; 21 (01) 203-211
- rong>?Bibi A, Java S, Chaudhary S. et al.?BRAFV600E?mutation in hairy cell leukemia: A single-center experience. Indian J Pathol Microbiol 2018; 61 (04) 532-536
- rong>?Pattnaik SA, Padhi S, Chhabra G. et al.?Atypical presentation of hairy cell leukemia: a report and comprehensive review. Blood Res 2020; 55 (02) 123-127
- rong>?Jain D, Dorwal P, Gajendra S, Pande A, Mehra S, Sachdev R.?CD5 positive hairy cell leukemia: a rare case report with brief review of literature. Cytometry B Clin Cytom 2016; 90 (05) 467-472
- rong>?Cortazar JM, DeAngelo DJ, Pinkus GS, Morgan EA.?Morphological and immunophenotypical features of hairy cell leukaemia involving lymph nodes and extranodal tissues. Histopathology 2017; 71 (01) 112-124
- rong>?Rahman ZA, Muwalla F, Jiang L, Foran J.?Hairy cell leukemia with CCND1/IGH fusion gene and BRAF V600E mutation. Leuk Res Rep 2020; 13: 100197
- rong>?Morgan EA, Katzman LE, Georgian-Smith D, Owings RA, Pinkus GS, Deangelo DJ.?Hairy cell leukemia presenting as a palpable breast mass. J Hematop 2014; 7: 181-187
- rong>?Miranda RN, Briggs RC, Kinney MC, Veno PA, Hammer RD, Cousar JB.?Immunohistochemical detection of cyclin D1 using optimized conditions is highly specific for mantle cell lymphoma and hairy cell leukemia. Mod Pathol 2000; 13 (12) 1308-1314
- rong>?Sherman MJ, Hanson CA, Hoyer JD.?An assessment of the usefulness of immunohistochemical stains in the diagnosis of hairy cell leukemia. Am J Clin Pathol 2011; 136 (03) 390-399
- trong>?Chen D, Ketterling RP, Hanson CA, Colgan JP, Zent CS, Viswanatha DS.?A case of hairy cell leukemia with CCND1-IGH@ translocation: indolent non-nodal mantle cell lymphoma revisited. Am J Surg Pathol 2011; 35 (07) 1080-1084
- trong>?Chai KL, Morris T, Bazargan A.?A case report of hairy cell leukemia: an unusual presentation. Ann Clin Case Rep 2017; 2: 1412
- Ishida F, Kitano K, Ichikawa N. et al.?Hairy cell leukemia with translocation (11;20)(q13;q11) and overexpression of cyclin D1. Leuk Res 1999; 23 (08) 763-765
Address for correspondence
Publication History
30 December 2021 (online)
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
|?Fig. 1Bone marrow trephine biopsy in hairy cell leukemia showing diffuse infiltrate of lymphoid cells with a perinuclear halo giving a ?fried egg? appearance (A). Hematoxylin and eosin staining. Characteristic lymphoid cells with circumferential fine hair like projection (inset, right lower) seen in peripheral blood (Leishman?Giemsa stain, ?400) (B). Diffuse infiltrating lymphoid cells displaying strong positive results for Annexin A1 antibody test. Cyclin D1 nuclear positivity in two of the cases (C) weak to intermediate, case no. 5 (D) strong, case no. 7 ([Supplementary Table S1]). The remainder of the cases were negative for cyclin D1 (peroxidase?antiperoxidase).
|?Fig. 2Flow cytometric immunophenotyping plots (in one of our cases) with the population of interest (B-cells) gated in red on CD19 versus side-scattered light (SSC). The neoplastic B-cells were positive for CD11c (bright), CD25 (bright), CD200, CD103, and CD123, thus diagnostic of hairy cell leukemia. Note the dim to moderate CD23 positivity in the CD19+ lymphoid cells as previously reported in the literature. These cells also express aberrant CD10 positivity on IHC (reproduced with permission from Pattnaik et al[3]).
References
- , Piukovics K, Borb?nyi Z, Demeter J, Bagdi E, Kren?cs L.?A comprehensive immunophenotypic marker analysis of hairy cell leukemia in paraffin-embedded bone marrow trephine biopsies?a tissue microarray study. Pathol Oncol Res 2015; 21 (01) 203-211
- ibi A, Java S, Chaudhary S. et al.?BRAFV600E?mutation in hairy cell leukemia: A single-center experience. Indian J Pathol Microbiol 2018; 61 (04) 532-536
- attnaik SA, Padhi S, Chhabra G. et al.?Atypical presentation of hairy cell leukemia: a report and comprehensive review. Blood Res 2020; 55 (02) 123-127
- ain D, Dorwal P, Gajendra S, Pande A, Mehra S, Sachdev R.?CD5 positive hairy cell leukemia: a rare case report with brief review of literature. Cytometry B Clin Cytom 2016; 90 (05) 467-472
- ortazar JM, DeAngelo DJ, Pinkus GS, Morgan EA.?Morphological and immunophenotypical features of hairy cell leukaemia involving lymph nodes and extranodal tissues. Histopathology 2017; 71 (01) 112-124
- ahman ZA, Muwalla F, Jiang L, Foran J.?Hairy cell leukemia with CCND1/IGH fusion gene and BRAF V600E mutation. Leuk Res Rep 2020; 13: 100197
- organ EA, Katzman LE, Georgian-Smith D, Owings RA, Pinkus GS, Deangelo DJ.?Hairy cell leukemia presenting as a palpable breast mass. J Hematop 2014; 7: 181-187
- iranda RN, Briggs RC, Kinney MC, Veno PA, Hammer RD, Cousar JB.?Immunohistochemical detection of cyclin D1 using optimized conditions is highly specific for mantle cell lymphoma and hairy cell leukemia. Mod Pathol 2000; 13 (12) 1308-1314
- herman MJ, Hanson CA, Hoyer JD.?An assessment of the usefulness of immunohistochemical stains in the diagnosis of hairy cell leukemia. Am J Clin Pathol 2011; 136 (03) 390-399
- Chen D, Ketterling RP, Hanson CA, Colgan JP, Zent CS, Viswanatha DS.?A case of hairy cell leukemia with CCND1-IGH@ translocation: indolent non-nodal mantle cell lymphoma revisited. Am J Surg Pathol 2011; 35 (07) 1080-1084
- Chai KL, Morris T, Bazargan A.?A case report of hairy cell leukemia: an unusual presentation. Ann Clin Case Rep 2017; 2: 1412
- Ishida F, Kitano K, Ichikawa N. et al.?Hairy cell leukemia with translocation (11;20)(q13;q11) and overexpression of cyclin D1. Leuk Res 1999; 23 (08) 763-765