 PDF
PDF  Views
Views  Share
Share


Hand Schuller Christian disease
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2011; 32(03): 183-184
DOI: DOI: 10.4103/0971-5851.92835

Publication History
Article published online:
06 August 2021
© 2011. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Sir,
A 43-year-old lady presented with progressively increasing multiple swellings over the scalp for two years and increased frequency of micturition and increased water intake for 6 months. There was no evidence of other systemic involvement. Computerized tomography (CT) of the brain showed multiple geographic punched-out lesions with nonsclerotic margins and beveled edges, associated with well-defined nonenhancing hypodense cystic lesions. The pituitary stalk appeared normal. She underwent excision biopsy of the right frontal skull lesion which was consistent with histiocytosis X.
Hand Schuller Christian disease (HSC) is one of the three components included in histiocytosis X, the other two being eosinophilic granuloma and Letterer-Siwe disease. This disease is primarily seen in infants and children and is rarely seen in adults. The classical triad of HSC disease – exophthalmos, diabetes insipidus, and calvarial lytic lesions – is seen only in one-third of patients.[1] CT scan is particularly helpful in detecting and defining the bony lesions and the soft tissue involvement. Both the outer and inner tables of the skull are involved with beveled edges and soft tissue masses [Figure 1].[2] Coalescence of lytic lesions gives a morphological appearance which is termed as “Geographic Skull” [Figure 2].[3] The bones involved are skull, ribs, pelvis, scapula, and mandible. Vertebrae and the appendages are less frequently involved. Optic atrophy, otitis media, and extrusion of teeth may occur as a result of adjacent bony involvement.[4] Systemic involvement of this disease includes hepatosplenomegaly, lymphadenopathy, dermatological, gastrointestinal tract, renal and pulmonary involvement. Central nervous system involvement includes convulsions, increased intracranial pressure, focal neurological deficits, mental retardation, hearing disturbance, and tremors. Involvement of the pituitary and hypothalamus may result in delay in sexual maturity and bone development, which is often seen in the pediatric age group.[5] The factors indicating the prognosis of this disease include the patient's age at presentation, extent of the systemic involvement, and response to treatment.[1]
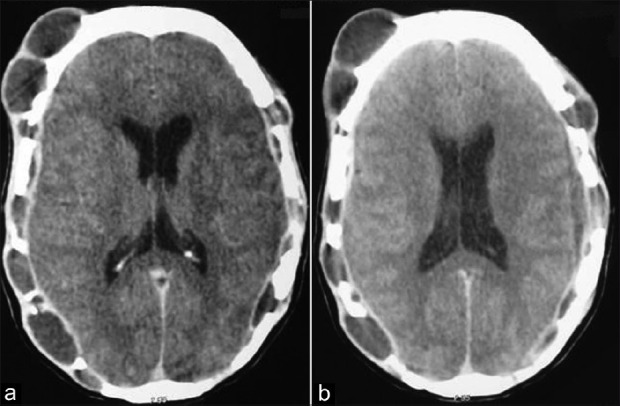
| Fig. 1 (a and b): CT scan of the brain axial views showing multiple lytic lesions of the cranium involving both inner and outer tables, with underlying normal brain parenchyma. Soft tissue masses seen overlying the pathological areas of the cranium
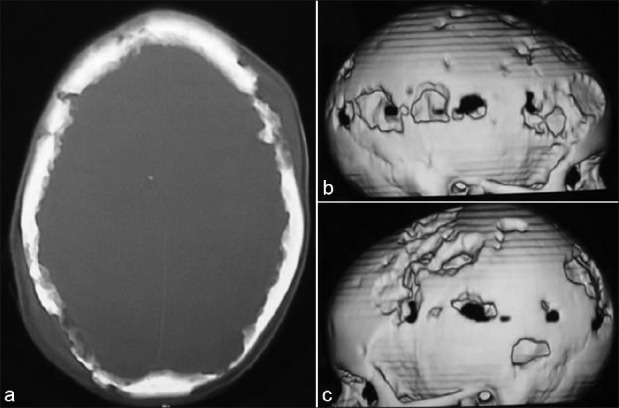
| Fig. 2: (a) CT scan of the cranial bone views showing multiple lytic lesions with beveled edges. (b-c) CT reconstruction of the bone showing the typical “Geographic Skull” appearance
REFERENCES
| Fig. 1 (a and b): CT scan of the brain axial views showing multiple lytic lesions of the cranium involving both inner and outer tables, with underlying normal brain parenchyma. Soft tissue masses seen overlying the pathological areas of the cranium
| Fig. 2: (a) CT scan of the cranial bone views showing multiple lytic lesions with beveled edges. (b-c) CT reconstruction of the bone showing the typical “Geographic Skull” appearance