 PDF
PDF  Views
Views  Share
Share


Pattern of Expression of CDX2 in Colorectal Cancer and its Role in Prognosis: An Ambispective Observational Study
CC BY 4.0 · Indian J Med Paediatr Oncol 2026; 47(02): 112-121
DOI: DOI: 10.1055/s-0042-1750207
Abstract
Introduction
Caudal-type homeobox 2 (CDX2), a nuclear protein, is essential for the proliferation and development of intestinal epithelial cells and is frequently downregulated during tumorigenesis. CDX2 inhibits cell growth as well as stimulates differentiation by activating intestinal specific genes, thus lack of CDX2 favors tumor growth and aggressiveness.
Objectives
We aimed to evaluate the pattern of CDX2 expression in all stages of colorectal cancer (CRC) and study its association with baseline characteristics and prognosis.
Materials and Methods
Study was conducted as an ambispective observational study, enrolling cases of CRC retrospectively from January 2014 to July 2016 (30 months), and prospectively during next 18-month period till January 2018. We performed CDX2 staining by immunohistochemistry on the available biopsy blocks of CRC patients during the study period. Total 286 patients were registered during the study period, of which only 110 biopsy blocks were available for staining. CDX2 scoring was done by a semiquantitative method on whole tissue section for the intensity and percentage of the cells showing positivity. Correlation of CDX2 expression was done with baseline clinical and histopathologic characteristics, and survival.
Results
Of 110 patients, 77 (70%) constituted colon cancer and 33 (30%) were rectal cancer. The median age was 54.2 years, 62 (56.4%) being male and 48 (43.6%) female with male-to-female ratio 1.3:1. In the study cohort, 33 (30%) patients had stage II disease, 30 (27.3%) stage III, and 47 (42.7%) were stage IV. Seventy-three (66.4%) were positive for CDX2 and 37 (33.4%) were negative. Loss of CDX2 expression was significantly associated with advanced stage, rectal site, poor grade of differentiation, and presence of lymphovascular invasion (LVSI). With median follow-up of 16 months, progression-free survival (PFS) at 2 years was 30% for CDX2 negative patients compared with 67% for CDX2 positive (p = 0.009), while overall survival (OS) at 2 years was 46% for CDX2 negative versus 77% for positive patients (p = 0.01).
Conclusion
Loss of CDX2 expression is associated with advanced stage, higher tumor grade, presence of LVSI, and worse PFS and OS and thereby functions as a poor prognostic factor in CRC.
Keywords
Authors' Contributions
Study concept and design: S.K., J.S., B.D., N.G.R. Provision of patient and study material: J.S., N.G.R., B.D., S.K., P.G., N.K.M., I.C. Performance and interpretation of IHC (immunohistochemistry): J.S., N.G.R., I.C. Data collection and analysis: J.S., N.G.R., S.K., B.D., K.K.M., I.C. Manuscript writing: J.S., S.K., B.D., P.G., N.G.R., N.K.M. Final approval of manuscript: all authors.
Note
The article has been read and approved by all authors. The requirements for authorship have been met, and all authors believe that the article represents honest work.
Justification for more than six authors: This study is an interdepartmental collaboration, initiated by the Department of Medical Oncology in conjunction with the Departments of Pathology and Surgery. Authorship has been assigned to all researchers who made substantial contributions to the work, in accordance with the ICMJE authorship criteria.
Publication History
28 November 2022
© 2022. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
A-13A, Graphix Tower 1, 6th floor, Sector 62, Noida 201309, Uttar Pradesh, India
We recommend
- Biomarkers of sequential progression in colorectal adenoma-dysplasia-carcinoma transition: gradual downregulation of amnionless homolog and prostaglandin D2 rec...O. Galamb, Zeitschrift für Gastroenterologie, 2008
- CDX2 Expression in Gastric Carcinoma: A Clinicopathological StudyAniket Halder, Mousumi Kundu, Ram Das, et al., TH Open, 2018
- New gene expression markers of colorectal adenoma-dysplasia-carcinoma sequenceO. Galamb, Zeitschrift für Gastroenterologie, 2007
- MUC2 and MUC5AC Expression in Colon Cancer: A Preliminary Report from South IndiaR Jayanth, Indian Journal of Medical and Paediatric Oncology, 2019
- HoxC8 expression in human colorectal cancer: a compensentory response of the cell to counter the transformation process?C. C. Schimanski, Zeitschrift für Gastroenterologie, 2005
- The development and implementation of pathological parameters and molecular testing impact prognosis of colorectal adenocarcinoma.Xu, Midie, Journal of the National Cancer Center, 2024
- Chemoprevention of colorectal cancer in individuals with previous colorectal neoplasia: systematic review and network meta-analysis<svg viewBox="0 0 24 24" fill="none" xmlns="http://www.w3.org/2000/svg">
</svg> by Mayo Clinic, The BMJ, 2016 - Colorectal cancerWilliam Hamilton, The BMJ, 2013
- MFAP2 promotes metastasis and drug resistance by regulating epithelial-to-mesenchymal transition through EGFR signaling pathway in colorectal cancer cells<svg viewBox="0 0 24 24" fill="none" xmlns="http://www.w3.org/2000/svg">
- ABC of colorectal diseases. Colorectal neoplasia--I: Benign colonic tumours.<svg viewBox="0 0 24 24" fill="none" xmlns="http://www.w3.org/2000/svg">
</svg> P. F. Schofield, The BMJ, 1992
Abstract
Introduction
Caudal-type homeobox 2 (CDX2), a nuclear protein, is essential for the proliferation and development of intestinal epithelial cells and is frequently downregulated during tumorigenesis. CDX2 inhibits cell growth as well as stimulates differentiation by activating intestinal specific genes, thus lack of CDX2 favors tumor growth and aggressiveness.
Objectives
We aimed to evaluate the pattern of CDX2 expression in all stages of colorectal cancer (CRC) and study its association with baseline characteristics and prognosis.
Materials and Methods
Study was conducted as an ambispective observational study, enrolling cases of CRC retrospectively from January 2014 to July 2016 (30 months), and prospectively during next 18-month period till January 2018. We performed CDX2 staining by immunohistochemistry on the available biopsy blocks of CRC patients during the study period. Total 286 patients were registered during the study period, of which only 110 biopsy blocks were available for staining. CDX2 scoring was done by a semiquantitative method on whole tissue section for the intensity and percentage of the cells showing positivity. Correlation of CDX2 expression was done with baseline clinical and histopathologic characteristics, and survival.
Results
Of 110 patients, 77 (70%) constituted colon cancer and 33 (30%) were rectal cancer. The median age was 54.2 years, 62 (56.4%) being male and 48 (43.6%) female with male-to-female ratio 1.3:1. In the study cohort, 33 (30%) patients had stage II disease, 30 (27.3%) stage III, and 47 (42.7%) were stage IV. Seventy-three (66.4%) were positive for CDX2 and 37 (33.4%) were negative. Loss of CDX2 expression was significantly associated with advanced stage, rectal site, poor grade of differentiation, and presence of lymphovascular invasion (LVSI). With median follow-up of 16 months, progression-free survival (PFS) at 2 years was 30%. for CDX2 negative patients compared with 67%. for CDX2 positive (p = 0.009), while overall survival (OS) at 2 years was 46%. for CDX2 negative versus 77%. for positive patients (p = 0.01).
Conclusion
Loss of CDX2 expression is associated with advanced stage, higher tumor grade, presence of LVSI, and worse PFS and OS and thereby functions as a poor prognostic factor in CRC.
Keywords
Introduction
Colorectal cancer (CRC) is one of the common cancers diagnosed worldwide and is considered as the second among the leading causes of cancer deaths.[1] The incidence and mortality from CRC is more in developed countries.[2] Approximately 20% of the patients with CRC presents with distant metastasis at diagnosis.[3]
Numerous prognostic markers, related to the pathogenesis of CRC have been studied to predict treatment outcome.[4] Several of these biomarkers are not reproducible and are not robust enough to find place in clinics. A few of these markers have come to clinical practice to help in knowing the prognosis and/or predicting response to particular therapy, either fluorouracil (5FU)/oxaliplatin-based chemotherapy or biological therapy. There is ongoing research to find more novel prognostic or predictive biomarkers or panel of markers at molecular levels to better stratify patients and determine systemic treatment based upon the risk groupings.[5]
Among the novel biomarkers, caudal-type homeobox 2 (CDX2) a nuclear transcription factor, has been explored to predict the survival outcomes in patients with CRC.[6] [7] CDX2 is an intestinal factor, encoded by CDX2 gene which is important for homeostasis and development of the intestinal epithelium.[8] CDX2 inhibits cell growth as well as stimulates differentiation by activating intestinal specific genes.[9] [10] Loss of CDX2 expression is seen in almost 30%. of human CRC and is associated with high tumor grade.[11] CDX2 expression can be identified both by gene expressing profile and immunohistochemistry (IHC).[12] A recent study has validated the prognostic and predictive utility of CDX2 in a large cohort of early-stage colon cancer.[13] Paucity of data on the role of CDX2 expression in advanced colon cancer, in rectal cancer, and in Indian population had surged us to undertake this work.
In our present study, we aimed to characterize the expression of CDX2 by IHC in all stages of colon as well as rectal cancers and to identify its association with various baseline clinical and histopathological parameters. Overall response rates (ORRs) and survival outcomes were evaluated in relation to CDX2 expression within the study cohort.
Material and Methods
Patient Recruitment and Data Collection
The study was conducted as an ambispective observational study. Cases were enrolled into the study both retrospectively (from January 2014 to July 2016; 30 months) and prospectively from July 2016 till January 2018 (18 months). Last case enrolled was followed up for a minimum of 6 months until the day of study analysis in July 2018. Cases enrolled into this study were identified from the central computerized database in the department of medical oncology at a tertiary cancer care center in South India. All newly diagnosed cases, age ≥ 18 years, any stage (early or advanced), with histopathologically proven diagnosis of CRC were considered for inclusion. Cases were excluded from the study if sufficient tissue material (either a biopsy or postoperative tissue blocks) was not available to perform IHC. Convenience sampling method was used for study enrollment and all consecutive cases meeting the inclusion/exclusion criteria registered during the study period were included into the study. Among 286 patients of CRC registered in the participating department during the study duration of January 2014 to January 2018, 110 cases met the inclusion criteria and were enrolled for analysis. Others (n = 176) were excluded due to unavailability of biopsy block or unstained slides.
Baseline clinical, histopathological, treatment, and follow-up details were collected from the medical file records. Baseline biopsies were reviewed for reconfirmation of pathological diagnosis for all eligible patients. Following outcome measures were considered for the study: primary measures: (1) percentage of CDX2 expression in the study cohort, (2) response rate in patients with advanced CRC, and (3) progression-free survival (PFS), and secondary outcome measures: (1) overall survival (OS).
Immunohistochemical Staining and Analysis of CDX2
Whole tissue section from the archived paraffin blocks were used and IHC staining for CDX2 was performed by using monoclonal mouse anti-human CDX2 (clone 88) (DAKO, USA) antibodies. Analysis of these was done by a semiquantitative method using a light microscope with a 40× objective at a total magnification of ×400. Area of interest (tumor cell regions avoiding areas containing fibrosis or necrosis) on stained slides was identified and representative 20 high power fields (HPF) were selected for scoring of the cell. The relative percentage of CDX2 positive cells in relation to overall cellularity was calculated for each HPF and the final score for an individual patient was taken as an average of the 20 HPF.
CDX2 Scoring
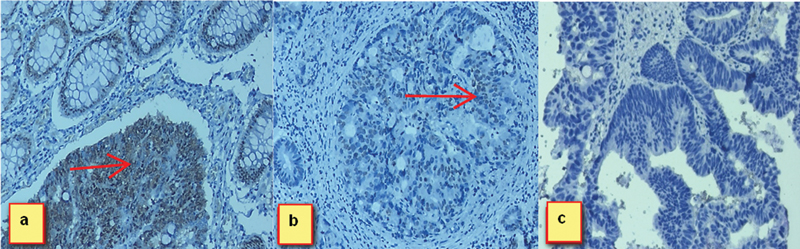
Fig 1:(A) Immunohistochemistry (IHC) stain, 40 × . Tumor cells show strong diffuse caudal-type homeobox 2 (CDX2) nuclear positivity along with normal intestinal mucosa. (B) IHC stain, 40 × . Focal weak nuclear CDX2 expression in tumor cells. (C) IHC stain, 40 × . Tumor cells are negative for CDX2
CDX2 scoring was done in semiquantitative method for the intensity and percentage of the cells showing positivity. Scoring was done according to the following pattern described by Bayrak et al[14]: “less than 5%. of tumor cells were given score of 0, 5 to 25%. of tumor cells positive for CDX2 considered as 1 + , 26 to 50%. of tumor cells positive for CDX2 as 2 + , 51 to 75%. of tumor cells positive for CDX2 were taken 3 + , and greater than 75%. of tumor cells positive for CDX2 as 4 + .” Additionally, positivity for CDX2 was also classified in the following subgroups: focal positivity if less than 50%. of tumor cells were positive and diffuse positivity staining in more than 50%. of the tumor cells.[14]
Statistical Analysis
Descriptive statistics was used for baseline characteristics, disease factors, laboratory, histopathological, treatment details, and CDX2 expression. Correlation of CDX2 expression with baseline clinical and histopathologic characteristics was done using chi-square test/Fisher's exact test for categorical data. Response rate with respect to CDX2 was calculated using chi-square test. Kaplan–Meier method was used for survival estimation and log-rank test was used for comparison. Median follow-up time for the cohort was calculated using the reverse Kaplan method for potential follow-up. Cox proportional hazards method was used to evaluate significance of CDX2 expression in predicting survival outcomes, while adjusting for other parameters with a significance level below 0.25 at a univariate level. Two-sided p-value of less than 0.05 was considered statistically significant. All statistical analysis was done using SPSS version 20.0 and data was censored on June 30, 2018 for survival analysis.
Endpoint definitions: PFS was defined as the time from initial diagnosis to progression at any time, relapse from complete response (CR), initiation of new previously unplanned treatment, or death from any cause. OS was defined as the time from date of registration till date of last follow-up or death from any cause. ORR for advanced stage CRC was defined as partial response or CR to chemotherapy according to response evaluation criteria in solid tumors (RECIST) criteria 1.1.[15]
Ethics: The study was approved by the institutional research and ethics committee (vide letter no. JIP/IEC/SC/2016/29/897 dated 12/07/2016). Informed consent was obtained from cases enrolled prospectively while a waiver of consent was granted for the retrospective cases. The procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation and with the Helsinki Declaration of 1964, as revised in 2013.
Results
A total of 110 cases were included into the study for analysis. Summary of the main results is described below.
Baseline Characteristics
|
Features |
Patients |
Total n = 110 |
||
|---|---|---|---|---|
|
Colon (77) |
Rectum (33) |
|||
|
1. |
Age (median age): 51.47 y (21–79 y) |
|||
|
(a) ≤ 30 y |
7 |
3 |
10 (9.1%) |
|
|
(b) 31–60 y |
47 |
20 |
67 (60.9%) |
|
|
(c) > 60 y |
23 |
10 |
33 (30%) |
|
|
2. |
Gender |
|||
|
(a) Male |
42 |
20 |
62 (56.4%) |
|
|
(b) Female |
35 |
13 |
48 (43.6%) |
|
|
3. |
Performance status |
|||
|
(a) 0–1 |
52 |
26 |
78 (70.9%) |
|
|
(b) 2 |
17 |
7 |
24 (21.8%) |
|
|
(c) 3 |
8 |
0 |
8 (7.3%) |
|
|
4. |
Site of disease |
|||
|
(a) Right colon |
38 |
− |
38 (34.5%) |
|
|
(b) Left colon |
39 |
− |
39 (35.5%) |
|
|
(c) Rectum |
− |
33 |
33 (30%) |
|
|
5. |
Stage of disease |
|||
|
(a) Stage II |
28 |
5 |
33 (30%) |
|
|
(b) Stage III |
21 |
9 |
30 (27.3%) |
|
|
(c) Stage IV |
28 |
19 |
47 (42.7%) |
|
|
6. |
Symptom duration (median): 3 mo (0–24 mo) |
|||
|
(a) < 1 mo |
13 |
2 |
15 (22.7%) |
|
|
(b) 1–6 mo |
50 |
25 |
75 (68.2%) |
|
|
(c) > 6 mo |
14 |
6 |
20 (18.1%) |
|
|
7. |
Symptoms[a] |
|||
|
(a) Obstruction and perforation |
12 |
1 |
13 (11.2%) |
|
|
(b) Abdominal pain/distension |
57 |
15 |
72 (62.1%) |
|
|
(c) Vomiting |
23 |
1 |
24 (20.7%) |
|
|
(d) Bleeding PR |
15 |
23 |
38 (32.8%) |
|
|
(e) Altered bowel habit |
10 |
8 |
18 (15.5%) |
|
|
(f) Decreased appetite/weight |
3 |
1 |
4 (3.4%) |
|
Abbreviations: CDX2, caudal-type homeobox 2; IQR, interquartile range.
Note: Median CDX2 positivity: 26.5%, IQR (1–70).
a In 37 patients who had negative CDX2 [removed]< 5>
Corelation of CDX2 with Baseline Parameters
Abbreviations: CDX2, caudal-type homeobox 2; LVSI, lymphovascular invasion; NACT, neoadjuvant chemotherapy; NACTRT, neoadjuvant chemoradiotherapy.
Treatment Particulars
Of 110 patients in the study, intent of treatment at baseline presentation was curative for 73 (66.4%) versus palliative for 37 (33.6%) patients. Definite surgery was done for 68.9% patients, 7.8%. had palliative surgery, and 23.3%. had no surgical intervention.
Ninety-seven (88.8%) received chemotherapy in the form neoadjuvant chemotherapy/chemoradiotherapy (n = 17, 17.5%), adjuvant chemotherapy (n = 50, 51.6%), or palliative chemotherapy (n = 30, 30.9%). The chemo regimens used were: combination of capecitabine plus oxaliplatin (CapeOX) in 67 (69.1%), combination of 5FU, leucovorin, and oxaliplatin (FOLFOX) in 13 (13.4%), single agent capecitabine in 16 (16.5%), and combination of 5FU, irinotecan, and leucovorin (FOLFIRI) in 1 (1%) patients. Thirty-six (37%) patients required dose modification and there was a delay of chemotherapy between the cycles in 40 (41.2%) patients for various reasons. Among 97 patients, 50 who received neoadjuvant chemotherapy/chemoradiotherapy or palliative chemotherapy were eligible for response assessment. Out of 50 eligible patients, responses were available for 41 (82%) patients. ORR was 19 (38%), 7 (14%) had stable disease and 15 (30%) had progressive disease while in 9 (18%) response was not available, as patients were lost to follow-up. Most common adverse effects with chemotherapy were hand-foot syndrome (n = 63, 61.2%), gastrointestinal (nausea; n = 64, 62.1%), and hematological (anemia; n = 45, 43.7%).
Survival Outcomes
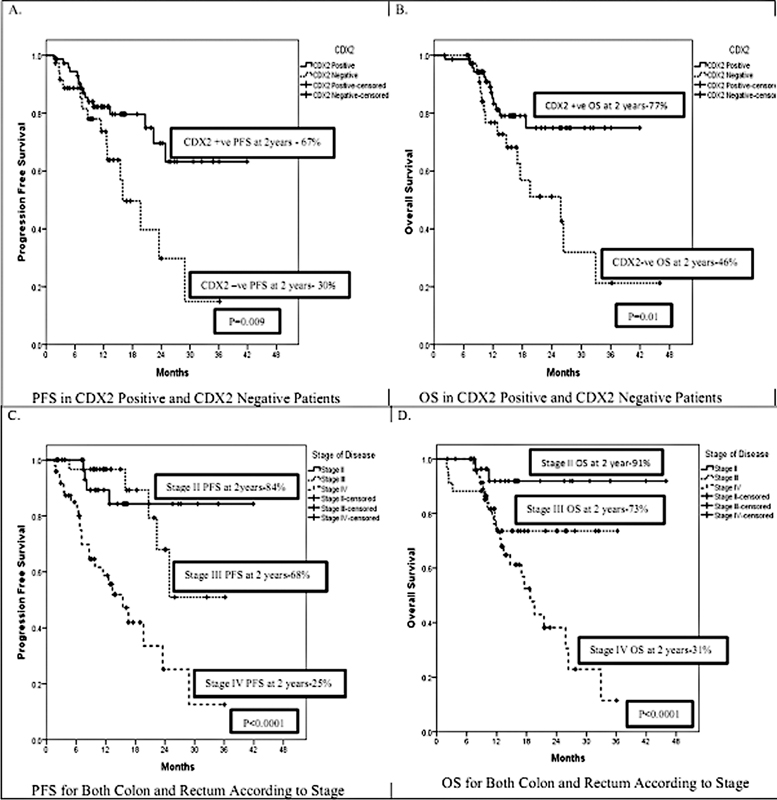
Fig 2 :(A) Progression-free survival for caudal-type homeobox 2 (CDX2) positive and negative patients. (B) Overall survival for CDX2 positive and negative patients. (C) Progression-free survival for stage II, III, and IV colorectal cancer. (D) Overall survival for stage II, III and IV colorectal cancer.
Factors Affecting Survival Outcome
Discussion
Risk stratification based upon prognostic markers is applied for treatment and predicting outcomes of CRCs. In early-stage colon cancer, higher grade, presence of obstruction or perforation, higher stage, and MMR deficiency are considered to harbor a poorer prognosis. Recently, CDX2, an intestine-specific nuclear transcription factor, has emerged as a new prognostic biomarker in CRC.[13] [16] [17] In this study, we identified the pattern of CDX2 expression in all the stages of CRC and have evaluated the association of CDX2 expression with baseline clinical and histopathological features, response to chemotherapy, and survival outcomes. Our study has shown that lack of CDX2 expression is associated with advanced stage, higher grade, presence of LVSI, and poorer PFS and OS.
CDX2, a nuclear protein expressed by the intestinal epithelium cells throughout the gut, is essential for the proliferation and growth of epithelial cells and is frequently downregulated during tumorigenesis.[18] [19] [20] Malignant progression of colorectal adenocarcinomas is characterized by the expression of oncoprotein β-catenin[21] [22] during tumor cell invasion and metastasis. CDX2 reduces the cellular proliferation and inhibits the β-catenin/T cell transcription factor transcriptional activity in colon cancer.[23] [24] Lack of CDX2 is associated with loss of differentiation of gastrointestinal epithelium leading to unregulated proliferation.[25] [26] [27] [28] Though the precise mechanisms for loss of CDX2 expression are not well characterized, low expression by IHC/gene expression has been associated with poorer prognosis, especially in early-stage CRC.[13] Since IHC is fast, reliable, and economical, we evaluated the pattern of expression of CDX2 by IHC in all stages of CRC and its association with prognosis.
There is variation in loss of CDX2 expression reported in different studies ranging from 4 to 30%, depending on the patient population, proportion of early and advanced stage colon cancers, proportion of rectal cancers, method for studying CDX2 (gene expression profile or IHC), tissue heterogeneity depending on use of tissue microarray or whole tissue section for IHC, and cutoff chosen for CDX2 positivity.[13] [16] [29] In our study, we have found a higher rate of loss of CDX2 [removed]33.6%) overall, possibly because of inclusion of patients with rectal cancers, a significant proportion of patients with stage IV disease, and use of whole tissue section for IHC. Our results are comparable to the study by Baba et al who reported loss of CDX2 in 29% of patient population of all stages of CRC.[16] Notably, CDX2 expression varies with the stage of CRC showing significantly low or loss of expression in advanced stage of the disease.[16] In our study around 2% of stage II CRC lacked CDX2 as compared with 6 and 25% of stage III and IV cases. In contrast to the study by Bae et al where female gender was associated with loss of CDX2 expression,[7] we did not find any significant association with age or gender, possibly due to population heterogeneity. Disease-related parameters like higher stage of disease, rectal site, higher grade of differentiation, and presence of LVSI were significantly associated with lack of CDX2 expression in our as well as in other studies.[7] [13] [16] [30] [31] [32] In our study, in patients receiving neoadjuvant or palliative chemotherapy, loss of CDX2 expression was not associated with response rate possibly due to small assessable number (n = 40) in this subgroup. Association of CDX2 expression with response rate to chemotherapy in the neoadjuvant or palliative setting has not been evaluated in any other study.
As CDX2 has an important role in impeding proliferation and promoting cellular differentiation,[33] loss of CDX2 expression is associated with poor outcomes. CDX2 loss contributes to aggressive disease behavior,[34] thereby increasing the likelihood of advanced stage.[35] In our study, loss of CDX2 in CRC patients was associated with both poor PFS and OS in univariate analysis, but no significance was seen in multivariate analysis possibly due to small sample size. Independent predictors of poor survival in multivariate analysis in our patient cohort were the widely established factors of advanced stage and higher grade. Independent prognostic effect of loss of CDX2 expression on survival outcomes has diverse results across studies. Results similar to our study of the significance of loss of CDX2 with poor survival outcomes in univariate but not in multivariate analysis in CRC was observed by Baba et al and Lugli et al,[16] [36] though other studies have shown that loss of CDX2 expression was independently associated with poor prognosis mostly in early-stage CRC.[7] [13] [37]
The limitations of our study were inclusion of a heterogeneous patient population, small sample size due to unavailability of many tissue blocks, some missing baseline information in the retrospective cohort, and short follow-up. Also, absence of MMR status for majority of cases was another main limitation. Use of whole tissue sections instead of tissue microarray, though labor-intensive, avoids tumor heterogeneity and false negative rates and this was one of the strengths of our study.
Conclusion
In conclusion, we found that loss of CDX2 expression is associated with markers of poor prognosis such as advanced disease stage, higher tumor grade, and presence of LVSI in CRC. Loss of CDX2 could possibly drive the evolution to poor biologic characteristics in the tumor. Loss of CDX2 was associated with worse PFS and OS in univariate analysis and our results attests its role as a poor prognostic factor in CRC. However, independent prognostic role of CDX2 in survival outcomes of CRC needs to be confirmed in larger multicenter data set with relatively longer follow-up.
Conflict of Interest
None declared.
Acknowledgment
We are thankful to the immunohistochemistry (IHC) section staff of Department of Pathology, JIPMER, Pondicherry for their help in carrying out the IHC staining.
Authors' Contributions
Study concept and design: S.K., J.S., B.D., N.G.R. Provision of patient and study material: J.S., N.G.R., B.D., S.K., P.G., N.K.M., I.C. Performance and interpretation of IHC (immunohistochemistry): J.S., N.G.R., I.C. Data collection and analysis: J.S., N.G.R., S.K., B.D., K.K.M., I.C. Manuscript writing: J.S., S.K., B.D., P.G., N.G.R., N.K.M. Final approval of manuscript: all authors.
Note
The article has been read and approved by all authors. The requirements for authorship have been met, and all authors believe that the article represents honest work.
Justification for more than six authors: This study is an interdepartmental collaboration, initiated by the Department of Medical Oncology in conjunction with the Departments of Pathology and Surgery. Authorship has been assigned to all researchers who made substantial contributions to the work, in accordance with the ICMJE authorship criteria.
References
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2018; 68 (06) 394-424
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin 2018; 68 (01) 7-30
- Cook AD, Single R, McCahill LE. Surgical resection of primary tumors in patients who present with stage IV colorectal cancer: an analysis of surveillance, epidemiology, and end results data, 1988 to 2000. Ann Surg Oncol 2005; 12 (08) 637-645
- George B, Kopetz S. Predictive and prognostic markers in colorectal cancer. Curr Oncol Rep 2011; 13 (03) 206-215
- Akiyoshi T, Kobunai T, Watanabe T. Recent approaches to identifying biomarkers for high-risk stage II colon cancer. Surg Today 2012; 42 (11) 1037-1045
- Zhang BY, Jones JC, Briggler AM. et al. Lack of caudal-type homeobox transcription factor 2 expression as a prognostic biomarker in metastatic colorectal cancer. Clin Colorectal Cancer 2017; 16 (02) 124-128
- Bae JM, Lee TH, Cho N-Y, Kim T-Y, Kang GH. Loss of CDX2 expression is associated with poor prognosis in colorectal cancer patients. World J Gastroenterol 2015; 21 (05) 1457-1467
- Freund JN, Domon-Dell C, Kedinger M, Duluc I. The Cdx-1 and Cdx-2 homeobox genes in the intestine. Biochem Cell Biol 1998; 76 (06) 957-969
- Suh E, Traber PG. An intestine-specific homeobox gene regulates proliferation and differentiation. Mol Cell Biol 1996; 16 (02) 619-625
- Almeida R, Silva E, Santos-Silva F. et al. Expression of intestine-specific transcription factors, CDX1 and CDX2, in intestinal metaplasia and gastric carcinomas. J Pathol 2003; 199 (01) 36-40
- Tóth C, Sükösd F, Valicsek E, Herpel E, Schirmacher P, Tiszlavicz L. Loss of CDX2 gene expression is associated with DNA repair proteins and is a crucial member of the Wnt signaling pathway in liver metastasis of colorectal cancer. Oncol Lett 2018; 15 (03) 3586-3593
- Witek ME, Nielsen K, Walters R. et al. The putative tumor suppressor Cdx2 is overexpressed by human colorectal adenocarcinomas. Clin Cancer Res 2005; 11 (24 Pt 1): 8549-8556
- Dalerba P, Sahoo D, Paik S. et al. CDX2 as a prognostic biomarker in stage II and stage III colon cancer. N Engl J Med 2016; 374 (03) 211-222
- Bayrak R, Haltas H, Yenidunya S. The value of CDX2 and cytokeratins 7 and 20 expression in differentiating colorectal adenocarcinomas from extraintestinal gastrointestinal adenocarcinomas: cytokeratin 7-/20+ phenotype is more specific than CDX2 antibody. Diagn Pathol 2012; 7: 9
- Schwartz LH, Litière S, de Vries E. et al. RECIST 1.1-update and clarification: from the RECIST committee. Eur J Cancer 2016; 62: 132-137
- Baba Y, Nosho K, Shima K. et al. Relationship of CDX2 loss with molecular features and prognosis in colorectal cancer. Clin Cancer Res 2009; 15 (14) 4665-4673
- Hinoi T, Tani M, Lucas PC. et al. Loss of CDX2 expression and microsatellite instability are prominent features of large cell minimally differentiated carcinomas of the colon. Am J Pathol 2001; 159 (06) 2239-2248
- Chawengsaksophak K, James R, Hammond VE, Köntgen F, Beck F. Homeosis and intestinal tumours in Cdx2 mutant mice. Nature 1997; 386 (6620): 84-87
- Beck F. The role of Cdx genes in the mammalian gut. Gut 2004; 53 (10) 1394-1396
- Mizoshita T, Inada K, Tsukamoto T. et al. Expression of Cdx1 and Cdx2 mRNAs and relevance of this expression to differentiation in human gastrointestinal mucosa–with special emphasis on participation in intestinal metaplasia of the human stomach. Gastric Cancer 2001; 4 (04) 185-191
- Morin PJ, Sparks AB, Korinek V. et al. Activation of beta-catenin-Tcf signaling in colon cancer by mutations in beta-catenin or APC. Science 1997; 275 (5307): 1787-1790
- Sparks AB, Morin PJ, Vogelstein B, Kinzler KW. Mutational analysis of the APC/beta-catenin/Tcf pathway in colorectal cancer. Cancer Res 1998; 58 (06) 1130-1134
- Guo R-J, Funakoshi S, Lee HH, Kong J, Lynch JP. The intestine-specific transcription factor Cdx2 inhibits beta-catenin/TCF transcriptional activity by disrupting the beta-catenin-TCF protein complex. Carcinogenesis 2010; 31 (02) 159-166
- Brabletz T, Jung A, Reu S. et al. Variable beta-catenin expression in colorectal cancers indicates tumor progression driven by the tumor environment. Proc Natl Acad Sci U S A 2001; 98 (18) 10356-10361
- Suh E, Chen L, Taylor J, Traber PG. A homeodomain protein related to caudal regulates intestine-specific gene transcription. Mol Cell Biol 1994; 14 (11) 7340-7351
- Bai Y-Q, Miyake S, Iwai T, Yuasa Y. CDX2, a homeobox transcription factor, upregulates transcription of the p21/WAF1/CIP1 gene. Oncogene 2003; 22 (39) 7942-7949
- Kaimaktchiev V, Terracciano L, Tornillo L. et al. The homeobox intestinal differentiation factor CDX2 is selectively expressed in gastrointestinal adenocarcinomas. Mod Pathol 2004; 17 (11) 1392-1399
- Bonhomme C, Duluc I, Martin E. et al. The Cdx2 homeobox gene has a tumour suppressor function in the distal colon in addition to a homeotic role during gut development. Gut 2003; 52 (10) 1465-1471
- Choi BJ, Kim CJ, Cho YG. et al. Altered expression of CDX2 in colorectal cancers. APMIS 2006; 114 (01) 50-54
- Kim GH, Lee DH, Kim HW. et al. Relationships between the expressions of CDX1 and CDX2 mRNA and clinicopathologic features in colorectal cancers. Korean J Intern Med (Korean Assoc Intern Med) 2005; 20 (04) 317-324
- Tomasello G, Barni S, Turati L. et al. Association of CDX2 expression with survival in early colorectal cancer: a systematic review and meta-analysis. Clin Colorectal Cancer 2018; 17 (02) 97-103
- Ryan ÉJ, Creavin B, Khaw YL. et al. Effects of CDX2 on prognosis and chemotherapy responsiveness in mismatch repair-deficient colorectal cancer. BJS Open 2018; 2 (06) 456-463
- Aoki K, Tamai Y, Horiike S, Oshima M, Taketo MM. Colonic polyposis caused by mTOR-mediated chromosomal instability in Apc+/Δ716 Cdx2+/- compound mutant mice. Nat Genet 2003; 35 (04) 323-330
- Hansel DE, Maitra A, Lin JW. et al. Expression of the caudal-type homeodomain transcription factors CDX 1/2 and outcome in carcinomas of the ampulla of Vater. J Clin Oncol 2005; 23 (09) 1811-1818
- Fan Z, Li J, Dong B, Huang X. Expression of Cdx2 and hepatocyte antigen in gastric carcinoma: correlation with histologic type and implications for prognosis. Clin Cancer Res 2005; 11 (17) 6162-6170
- Lugli A, Tzankov A, Zlobec I, Terracciano LM. Differential diagnostic and functional role of the multi-marker phenotype CDX2/CK20/CK7 in colorectal cancer stratified by mismatch repair status. Mod Pathol 2008; 21 (11) 1403-1412
- Dawson H, Koelzer VH, Lukesch AC. et al. Loss of Cdx2 expression in primary tumors and lymph node metastases is specific for mismatch repair-deficiency in colorectal cancer. Front Oncol 2013; 3: 265
Address for correspondence
Publication History
Article published online:
28 November 2022
© 2022. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Private Limited
A-13A, Graphix Tower 1, 6th floor, Sector 62, Noida 201309, Uttar Pradesh, India
We recommend
- Biomarkers of sequential progression in colorectal adenoma-dysplasia-carcinoma transition: gradual downregulation of amnionless homolog and prostaglandin D2 rec...O. Galamb, Zeitschrift für Gastroenterologie, 2008
- CDX2 Expression in Gastric Carcinoma: A Clinicopathological StudyAniket Halder, Mousumi Kundu, Ram Das, et al., Indian Journal of Medical and Paediatric Oncology, 2018
- New gene expression markers of colorectal adenoma-dysplasia-carcinoma sequenceO. Galamb, Zeitschrift für Gastroenterologie, 2007
- MUC2 and MUC5AC Expression in Colon Cancer: A Preliminary Report from South IndiaR Jayanth, Indian Journal of Medical and Paediatric Oncology, 2019
- HoxC8 expression in human colorectal cancer: a compensentory response of the cell to counter the transformation process?C. C. Schimanski, Zeitschrift für Gastroenterologie, 2005
- Effects of CDX2 on prognosis and chemotherapy responsiveness in mismatch repair-deficient colorectal cancerBJS Open, 2018
- Sidedness Matters: Surrogate Biomarkers Prognosticate Colorectal Cancer upon Anatomic LocationIrit Ben‐Aharon, The Oncologist, 2019
- DUOX2 promotes the progression of colorectal cancer cells by regulating the AKT pathway and interacting with RPL3Xue Zhang, Carcinogenesis, 2020
- Immunohistochemistry‐Based Consensus Molecular Subtypes as a Prognostic and Predictive Biomarker for Adjuvant Chemotherapy in Patients with Stage II Colorectal ...Yaqi Li, The Oncologist, 2020
- P463 Crohn’s disease–associated anorectal cancer has a poor prognosis with high local recurrence: a subanalysis of the Nationwide Japanese StudyT Ogino, Journal of Crohn's and Colitis, 2023
References
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2018; 68 (06) 394-424
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin 2018; 68 (01) 7-30
- Cook AD, Single R, McCahill LE. Surgical resection of primary tumors in patients who present with stage IV colorectal cancer: an analysis of surveillance, epidemiology, and end results data, 1988 to 2000. Ann Surg Oncol 2005; 12 (08) 637-645
- George B, Kopetz S. Predictive and prognostic markers in colorectal cancer. Curr Oncol Rep 2011; 13 (03) 206-215
- Akiyoshi T, Kobunai T, Watanabe T. Recent approaches to identifying biomarkers for high-risk stage II colon cancer. Surg Today 2012; 42 (11) 1037-1045
- Zhang BY, Jones JC, Briggler AM. et al. Lack of caudal-type homeobox transcription factor 2 expression as a prognostic biomarker in metastatic colorectal cancer. Clin Colorectal Cancer 2017; 16 (02) 124-128
- Bae JM, Lee TH, Cho N-Y, Kim T-Y, Kang GH. Loss of CDX2 expression is associated with poor prognosis in colorectal cancer patients. World J Gastroenterol 2015; 21 (05) 1457-1467
- Freund JN, Domon-Dell C, Kedinger M, Duluc I. The Cdx-1 and Cdx-2 homeobox genes in the intestine. Biochem Cell Biol 1998; 76 (06) 957-969
- Suh E, Traber PG. An intestine-specific homeobox gene regulates proliferation and differentiation. Mol Cell Biol 1996; 16 (02) 619-625
- Almeida R, Silva E, Santos-Silva F. et al. Expression of intestine-specific transcription factors, CDX1 and CDX2, in intestinal metaplasia and gastric carcinomas. J Pathol 2003; 199 (01) 36-40
- Tóth C, Sükösd F, Valicsek E, Herpel E, Schirmacher P, Tiszlavicz L. Loss of CDX2 gene expression is associated with DNA repair proteins and is a crucial member of the Wnt signaling pathway in liver metastasis of colorectal cancer. Oncol Lett 2018; 15 (03) 3586-3593
- Witek ME, Nielsen K, Walters R. et al. The putative tumor suppressor Cdx2 is overexpressed by human colorectal adenocarcinomas. Clin Cancer Res 2005; 11 (24 Pt 1): 8549-8556
- Dalerba P, Sahoo D, Paik S. et al. CDX2 as a prognostic biomarker in stage II and stage III colon cancer. N Engl J Med 2016; 374 (03) 211-222
- Bayrak R, Haltas H, Yenidunya S. The value of CDX2 and cytokeratins 7 and 20 expression in differentiating colorectal adenocarcinomas from extraintestinal gastrointestinal adenocarcinomas: cytokeratin 7-/20+ phenotype is more specific than CDX2 antibody. Diagn Pathol 2012; 7: 9
- Schwartz LH, Litière S, de Vries E. et al. RECIST 1.1-update and clarification: from the RECIST committee. Eur J Cancer 2016; 62: 132-137
- Baba Y, Nosho K, Shima K. et al. Relationship of CDX2 loss with molecular features and prognosis in colorectal cancer. Clin Cancer Res 2009; 15 (14) 4665-4673
- Hinoi T, Tani M, Lucas PC. et al. Loss of CDX2 expression and microsatellite instability are prominent features of large cell minimally differentiated carcinomas of the colon. Am J Pathol 2001; 159 (06) 2239-2248
- Chawengsaksophak K, James R, Hammond VE, Köntgen F, Beck F. Homeosis and intestinal tumours in Cdx2 mutant mice. Nature 1997; 386 (6620): 84-87
- Beck F. The role of Cdx genes in the mammalian gut. Gut 2004; 53 (10) 1394-1396
- Mizoshita T, Inada K, Tsukamoto T. et al. Expression of Cdx1 and Cdx2 mRNAs and relevance of this expression to differentiation in human gastrointestinal mucosa–with special emphasis on participation in intestinal metaplasia of the human stomach. Gastric Cancer 2001; 4 (04) 185-191
- Morin PJ, Sparks AB, Korinek V. et al. Activation of beta-catenin-Tcf signaling in colon cancer by mutations in beta-catenin or APC. Science 1997; 275 (5307): 1787-1790
- Sparks AB, Morin PJ, Vogelstein B, Kinzler KW. Mutational analysis of the APC/beta-catenin/Tcf pathway in colorectal cancer. Cancer Res 1998; 58 (06) 1130-1134
- Guo R-J, Funakoshi S, Lee HH, Kong J, Lynch JP. The intestine-specific transcription factor Cdx2 inhibits beta-catenin/TCF transcriptional activity by disrupting the beta-catenin-TCF protein complex. Carcinogenesis 2010; 31 (02) 159-166
- Brabletz T, Jung A, Reu S. et al. Variable beta-catenin expression in colorectal cancers indicates tumor progression driven by the tumor environment. Proc Natl Acad Sci U S A 2001; 98 (18) 10356-10361
- Suh E, Chen L, Taylor J, Traber PG. A homeodomain protein related to caudal regulates intestine-specific gene transcription. Mol Cell Biol 1994; 14 (11) 7340-7351
- Bai Y-Q, Miyake S, Iwai T, Yuasa Y. CDX2, a homeobox transcription factor, upregulates transcription of the p21/WAF1/CIP1 gene. Oncogene 2003; 22 (39) 7942-7949
- Kaimaktchiev V, Terracciano L, Tornillo L. et al. The homeobox intestinal differentiation factor CDX2 is selectively expressed in gastrointestinal adenocarcinomas. Mod Pathol 2004; 17 (11) 1392-1399
- Bonhomme C, Duluc I, Martin E. et al. The Cdx2 homeobox gene has a tumour suppressor function in the distal colon in addition to a homeotic role during gut development. Gut 2003; 52 (10) 1465-1471
- Choi BJ, Kim CJ, Cho YG. et al. Altered expression of CDX2 in colorectal cancers. APMIS 2006; 114 (01) 50-54
- Kim GH, Lee DH, Kim HW. et al. Relationships between the expressions of CDX1 and CDX2 mRNA and clinicopathologic features in colorectal cancers. Korean J Intern Med (Korean Assoc Intern Med) 2005; 20 (04) 317-324
- Tomasello G, Barni S, Turati L. et al. Association of CDX2 expression with survival in early colorectal cancer: a systematic review and meta-analysis. Clin Colorectal Cancer 2018; 17 (02) 97-103
- Ryan ÉJ, Creavin B, Khaw YL. et al. Effects of CDX2 on prognosis and chemotherapy responsiveness in mismatch repair-deficient colorectal cancer. BJS Open 2018; 2 (06) 456-463
- Aoki K, Tamai Y, Horiike S, Oshima M, Taketo MM. Colonic polyposis caused by mTOR-mediated chromosomal instability in Apc+/Δ716 Cdx2+/- compound mutant mice. Nat Genet 2003; 35 (04) 323-330
- Hansel DE, Maitra A, Lin JW. et al. Expression of the caudal-type homeodomain transcription factors CDX 1/2 and outcome in carcinomas of the ampulla of Vater. J Clin Oncol 2005; 23 (09) 1811-1818
- Fan Z, Li J, Dong B, Huang X. Expression of Cdx2 and hepatocyte antigen in gastric carcinoma: correlation with histologic type and implications for prognosis. Clin Cancer Res 2005; 11 (17) 6162-6170
- Lugli A, Tzankov A, Zlobec I, Terracciano LM. Differential diagnostic and functional role of the multi-marker phenotype CDX2/CK20/CK7 in colorectal cancer stratified by mismatch repair status. Mod Pathol 2008; 21 (11) 1403-1412
- Dawson H, Koelzer VH, Lukesch AC. et al. Loss of Cdx2 expression in primary tumors and lymph node metastases is specific for mismatch repair-deficiency in colorectal cancer. Front Oncol 2013; 3: 265