 PDF
PDF  Views
Views  Share
Share


Two Cases of Acinic Cell Carcinoma of Parotid Gland – Rare Papillary Cystic Variant: One Unusual Presentation in Older Male Patient
CC BY-NC-ND 4.0 · Indian J Med Paediatr Oncol 2017; 38(02): 242-244
DOI: DOI: 10.4103/ijmpo.ijmpo_39_16
|
Publication History
Article published online:
06 July 2021
© 2017. Indian Society of Medical and Paediatric Oncology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/.)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
Sir,
Papillary cystic variant of acinic cell carcinoma (ACC-PCV) is an uncommon tumor that has been mostly reported to occur in younger patients (16–40 years) as compared to the classic type that characteristically presents in the fifth decade of life.
We are reporting two cases of this rare entity ACC-PCV which came to our institute for review of slides at the age of 15 and 49 years of age, respectively, and was given diagnosis as ACC-PCV. However, the case 2 in our presentation is unusual itself in this rare entity, as presenting in older male patient. ACC-PCV variant has a poorer prognosis.
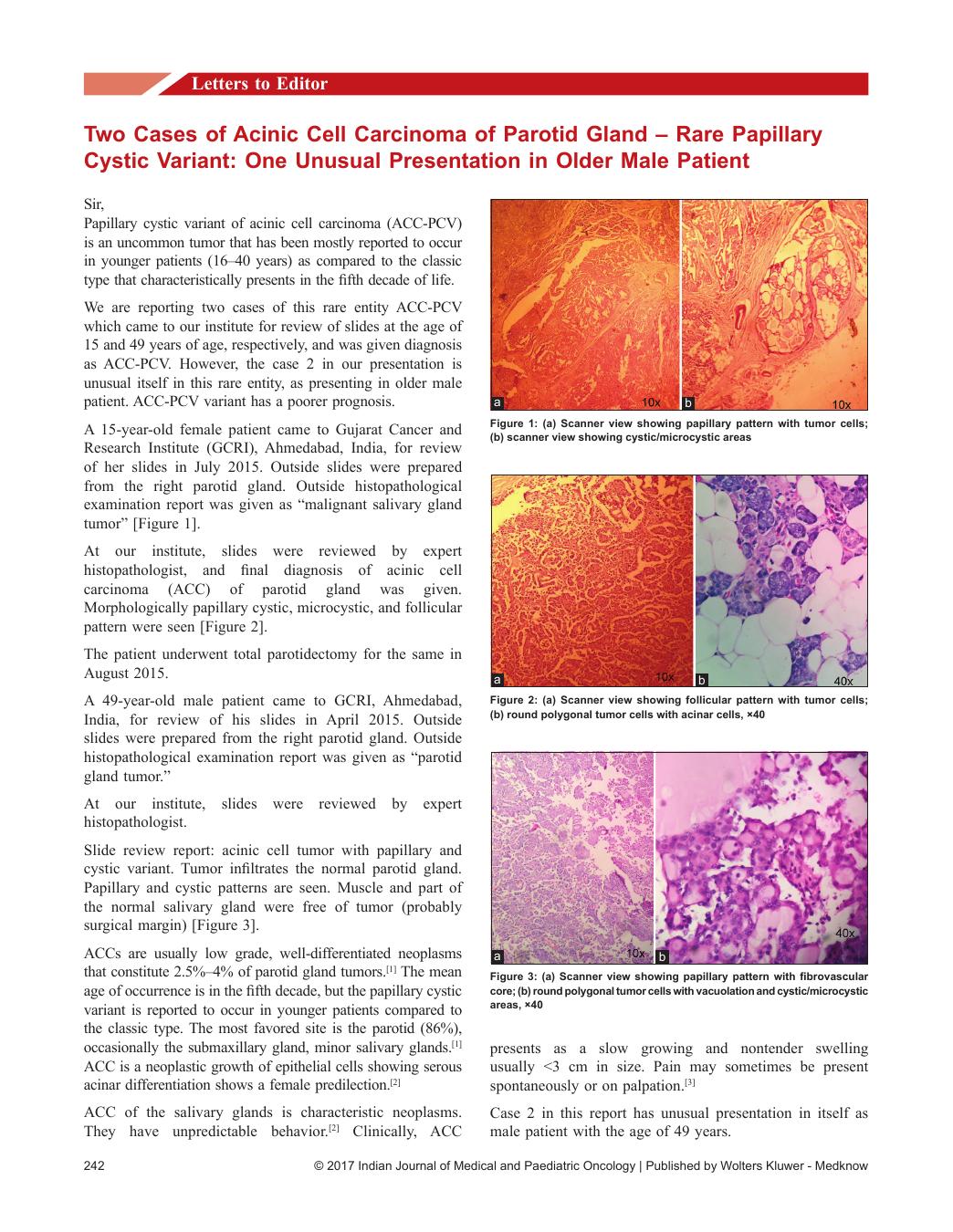
A 15-year-old female patient came to Gujarat Cancer and Research Institute (GCRI), Ahmedabad, India, for review of her slides in July 2015. Outside slides were prepared from the right parotid gland. Outside histopathological examination report was given as “malignant salivary gland tumor” [Figure 1].
| Figure 1:(a) Scanner view showing papillary pattern with tumor cells; (b) scanner view showing cystic/microcystic areas
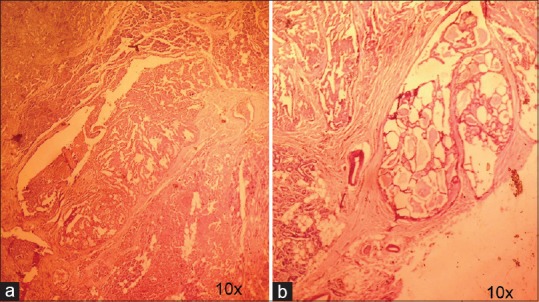
At our institute, slides were reviewed by expert histopathologist, and final diagnosis of acinic cell carcinoma (ACC) of parotid gland was given. Morphologically papillary cystic, microcystic, and follicular pattern were seen [Figure 2].
| Figure 2:(a) Scanner view showing follicular pattern with tumor cells; (b) round polygonal tumor cells with acinar cells, ×40
The patient underwent total parotidectomy for the same in August 2015.
A 49-year-old male patient came to GCRI, Ahmedabad, India, for review of his slides in April 2015. Outside slides were prepared from the right parotid gland. Outside histopathological examination report was given as “parotid gland tumor.”
At our institute, slides were reviewed by expert histopathologist.
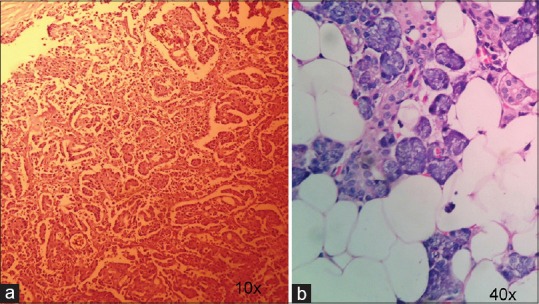
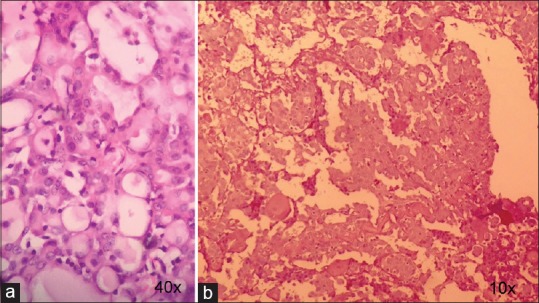
Slide review report: acinic cell tumor with papillary and cystic variant. Tumor infiltrates the normal parotid gland. Papillary and cystic patterns are seen. Muscle and part of the normal salivary gland were free of tumor (probably surgical margin) [Figure 3].
| Figure 3:(a) Scanner view showing papillary pattern with fibrovascular core; (b) round polygonal tumor cells with vacuolation and cystic/microcystic areas, ×40
ACCs are usually low grade, well-differentiated neoplasms that constitute 2.5%–4% of parotid gland tumors.[1] The mean age of occurrence is in the fifth decade, but the papillary cystic variant is reported to occur in younger patients compared to the classic type. The most favored site is the parotid (86%), occasionally the submaxillary gland, minor salivary glands.[1] ACC is a neoplastic growth of epithelial cells showing serous acinar differentiation shows a female predilection.[2]
ACC of the salivary glands is characteristic neoplasms. They have unpredictable behavior.[2] Clinically, ACC presents as a slow growing and nontender swelling usually <3 href="https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5582572/#ref3" rid="ref3" class=" bibr popnode" role="button" aria-expanded="false" aria-haspopup="true" xss=removed>3]
Case 2 in this report has unusual presentation in itself as male patient with the age of 49 years.
ACC-PCV is histologically composed of tumor with papillary and cystic growth patterns, with varying proportions of one or more cell types. It has the significance because it has a poorer prognosis. In addition to that, it is reported to be universally fatal in 10 years.
Numerous reasons have been given for difficulty in cytodiagnosis:[3]
- Cystic fluid dilutes the overall cellularity leading to a benign diagnosis
- Cytoarchitecture is different from classic type – prominent papillary architecture with more cohesive cells with high nuclear-cytoplasmic ratio
- Change in morphology of tumor cells due to suspension in cystic fluid
- The presence of metaplastic oncocytic or squamoid changes either focally or otherwise.
The diagnosis of ACC-PCV is easy on histology.[4] However, the cytological diagnosis is a problem because of the cytoarchitecture which is different from classic type.[5] Misinterpretation of diagnosis may occur due to lack of experience in dealing with this tumor type and very few published literature on ACC-PCV. ACC-PCV cases have different appearance of the tumor resembling other benign and malignant salivary gland lesions.
Usually, ACC-PCV is an encapsulated and capsular invasion is a common finding on microscopy. It displays papillary folds interspersed with cystic spaces.
ACC-papillary cystic variant is histologically composed of tumor with papillary and cystic growth patterns, with varying proportions of one or more of five cell types which include “hobnail” acinar, intercalated, vacuolated, nonspecific glandular, and clear cells.[2]
The clinical picture is not specific, and diagnosis is based on the histopathologic examination.[2]
The papillary cystic variant is believed to have two forms of genesis: One a retrogressive phenomenon; the other solely neoplastic.[3] The former is a histopathologic reflection of a self-destructive quality of some ACCs, the end stage of which is a solitary loculated cyst with attenuated and hydropically altered neoplastic cells in company with neoplastic papillary excrescences in various stages of degeneration.[3]
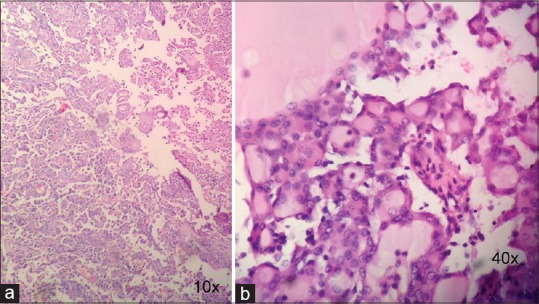
Histopathologically, a distinct fibrous connective tissue usually encapsulates the tumor, but marginal infiltration is a prominent feature. The tumor is composed of diverse cell types, and these are acinic cells, vacuolated cells, intercalated cells, nonspecific glandular cells, and clear cells. Thirteen acinic cells resemble the polyhedral cells of normal acini and contain abundant finely granular cytoplasm which may be basophilic, amphophilic, or pale eosinophilic. Nuclei are generally small, regular, hyperchromatic with a prominent nucleolus. Characteristic cytoplasmic granularity with strongly PAS and D-PAS positive granules is seen [Figure 4].
| Figure 4:(a) Acinar tumor cells with vacuolation, ×40; (b) scanner view showing periodic acid–Schiff positive secretions and granules
Intercalated cells are cuboidal cells with limited amphophilic cytoplasm, distinct borders. Vacuolated cells are characterized by one or two large or multiple vacuoles. In our cases, vacuolation was seen predominantly. Nonspecific glandular cells, lack specific glandular features, have a faintly eosinophilic or amphophilic cytoplasm, and no granules.[2]
Characteristically seen in papillary-cystic variant, they have a tendency to form “hobnail cells,” presumably after releasing their secretions into glandular spaces. Clear cells are characterized by their nonstainable cytoplasm and distinct nondistended cell borders.[2]
The different architectural patterns which may be seen in ACC are solid, solid-lobular, acinar-microcystic, papillary cystic, tubuloductal, follicular/macrocystic, and dedifferentiated. Although a single pattern usually dominates, a mixture of histologic patterns may also be observed.
The case 1 is showing mixture of histologic patterns.
Papillary-cystic typically involves the transition of usual dense cellularity into papillary folds interspersed with cystic spaces. It may vary from small cysts with scanty papillary projections to large cystic spaces into which extend delicate papillary growths supported by thin, vascular stalks.
Follicular/macrocystic pattern demonstrates follicular arrangement of cells with centrally located, pink, homogeneous, colloid-like material resembling thyroid follicles.
Microcystic pattern exhibits intercellular spaces formed due to coalescence of intracellular vacuoles.
The case 2 is showing papillary and cystic patterns.
The choice of treatment is total parotidectomy.
The most significant differential diagnosis of ACC-PCV is papillary carcinoma of the thyroid. Thyroid ultrasonography hormonal assays and immunohistochemistry for thyroglobulin help in differentiating the two.[3]
As ACC-PCV usually presents in younger age with female preponderance. Our case 2 male patient at 49 years shows the unusual presentation.
Other less significant differential diagnosis includes cystadenocarcinoma and polymorphous low-grade adenocarcinoma. Metastasis is rare in cases of ACC-PCV. Timely diagnosis and treatment are essential as ACC-PCV has been found to be universally fatal in 10 years.[5]
Hence, oncologists should keep ACC-PCV as a possibility in mind while coming across relevant cases, and oncologists should test such patients for histopathological examination, as clinical picture is inconclusive. Pathologists have the responsibility to reach to a final diagnosis.
Financial support and sponsorshipNil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
We all authors would like to thank Dr. R. K. Vyas, Director of Gujarat Cancer and Research Institute, Ahmedabad, Gujarat, India, to allow us to publish this article.
References
- Jayaram G, Othman MA, Kumar M, Krishnan G. Papillary cystic type of acinic cell carcinoma of parotid: Fine needle aspiration cytological features of a high grade variant with oncocytic metaplasia. Malays J Pathol 2002;24:107-12.
- Shah A, Patwari M, Deshmukh RS. Acinic cell carcinoma, papillary-cystic variant of the parotid gland: A case report with review of literature. Oral Oncol Extra 2005;41:137-41.
- Augustine J, Kumar P, Saran RK, Mohanty S. Papillary cystic acinic cell carcinoma: Report of a rare lesion with unusual presentation. J Clin Exp Dent 2011;3:e169-71.
- Narayan SM, Padmini J, Parthiban R, Madhusmita J, Natarajan G, Revadi PS. Diagnosis of a case of papillary-cystic variant of acinic-cell carcinoma on fine needle aspiration cytology: Myriad of cytomorphological features. Int J Case Rep Imag 2014;5:18-22. [Doi: 10.5348/ijcri-2014-01-431-CR-4].
- Ali SZ. Acinic-cell carcinoma, papillary-cystic variant: A diagnostic dilemma in salivary gland aspiration. Diagn Cytopathol 2002;27:244-50.
| Figure 1:(a) Scanner view showing papillary pattern with tumor cells; (b) scanner view showing cystic/microcystic areas
| Figure 2:(a) Scanner view showing follicular pattern with tumor cells; (b) round polygonal tumor cells with acinar cells, ×40
| Figure 3:(a) Scanner view showing papillary pattern with fibrovascular core; (b) round polygonal tumor cells with vacuolation and cystic/microcystic areas, ×40
| Figure 4:(a) Acinar tumor cells with vacuolation, ×40; (b) scanner view showing periodic acid–Schiff positive secretions and granules
References
- Jayaram G, Othman MA, Kumar M, Krishnan G. Papillary cystic type of acinic cell carcinoma of parotid: Fine needle aspiration cytological features of a high grade variant with oncocytic metaplasia. Malays J Pathol 2002;24:107-12.
- Shah A, Patwari M, Deshmukh RS. Acinic cell carcinoma, papillary-cystic variant of the parotid gland: A case report with review of literature. Oral Oncol Extra 2005;41:137-41.
- Augustine J, Kumar P, Saran RK, Mohanty S. Papillary cystic acinic cell carcinoma: Report of a rare lesion with unusual presentation. J Clin Exp Dent 2011;3:e169-71.
- Narayan SM, Padmini J, Parthiban R, Madhusmita J, Natarajan G, Revadi PS. Diagnosis of a case of papillary-cystic variant of acinic-cell carcinoma on fine needle aspiration cytology: Myriad of cytomorphological features. Int J Case Rep Imag 2014;5:18-22. [Doi: 10.5348/ijcri-2014-01-431-CR-4].
- Ali SZ. Acinic-cell carcinoma, papillary-cystic variant: A diagnostic dilemma in salivary gland aspiration. Diagn Cytopathol 2002;27:244-50.